IJCRR - 5(17), September, 2013
Pages: 54-56
Date of Publication: 12-Sep-2013
Print Article
Download XML Download PDF
VALUE OF REPEAT PLAIN X-RAY ABDOMEN IN DUODENAL PERFORATION
Author: M. Palaniappan, C. P. Ganesh Babu, M. Balachandar
Category: Healthcare
Abstract:Aim: To highlight the value of repeat plain X ray abdomen in duodenal ulcer perforation. Case report: 60 year old female patient was admitted with duodenal perforation with negative X-ray at the time of admission. Later the same investigation revealed pneumoperitoneum. Discussion: Pneumoperitoneum may not be evident in all duodenal ulcer perforations immediately after admission. In such occasions, repeat plain X ray abdomen may clinch the diagnosis. Conclusion: The value of repeat X-ray in suspected cases of perforation is stressed in this case scenario.
Keywords: duodenal ulcer perforation, repeat plain X ray abdomen
Full Text:
INTRODUCTION
Duodenal ulcer perforation is one of the commonest emergencies done in general surgery. Clinical diagnosis is made by signs of peritonitis and liver dullness obliteration. Plain x-ray abdomen usually reveals air under diaphragm.In a few patients x-ray does not reveal pneumoperitoneum. In such patients, repeat x-ray turns out to be valuable.
CASE REPORT
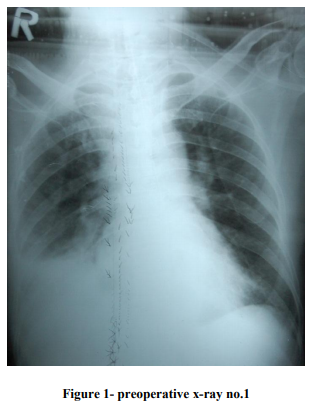
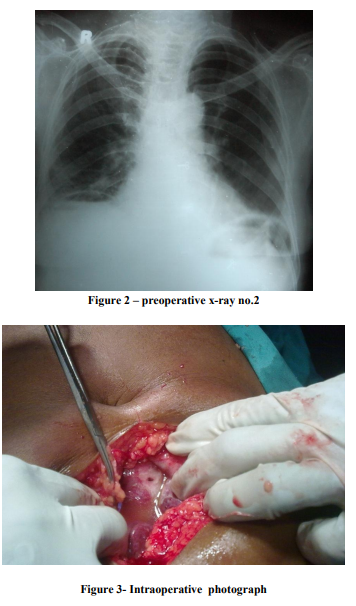
Chellammal, 60 years lady presented with complaints of severe generalised abdominal pain of sudden onset of one day duration. She had no previous history of peptic ulcer. On examination, the clinical picture was that of peritonitis. Plain xray abdomen soon after admission showed no pneumoperitoneum. (Fig 1) Patient was put on drip, Ryles tube aspiration and antibiotics. In the course of resuscitation, after 4 hours, a second plain x-ray abdomen was taken which showed gas under the diaphragm.(Fig 2) Hence clinical suspicion of perforated hollow viscus was confirmed. At emergency laparotomy, a 2mm duodenal perforation was found(Fig 3) in the anterior wall of the first part of duodenum. This was closed by sutures with live omental patch reinforcement. In the subsequent post-operative course, patient did well. She was discharged early in the third week after complete wound healing.
DISCUSSION
Diagnosis of perforative peritonitis is usually straightforward. X-ray findings are confirmatory with pneumoperitoneum. In a few patients x-ray does not support the clinical findings. Small quantities of free gas, as little as 1cc are best detected on erect chest and left lateral decubitus films, according to Miller and colleagues in 1980(1) Air insufflation via Ryles tube has been advocated by some to reveal pneumoperitoneum in duodenal perforation. Gastrograffin dye instillation through Ryles tube and x-ray to reveal dye leak has also been suggested. (2) But in our opinion, these procedures carry the risk of reopening spontaneous seal of a perforation and adversely affecting the outcome. A simple repeat plain x-ray abdomen after 3 or 4 hours in the course of resuscitation is very safe, simple, easy to carry out and informative in patients with acute abdomen.
CONCLUSION
Various methods have been suggested for confirming pneumoperitonium in patients with negative X rays, like injecting air through the Ryle’s tube before X ray or taking contrast X ray. But simple repeat plain Xray abdomen after three or four hours is the safest and simplest method without risk of reopening spontaneously sealed perforations. In patients with peritonitis if the initial x-ray is not informative ,during the course of resuscitation repeat plain x-ray in 3 or 4 hours can be valuable. This article emphasises the value of simple repeat plain x-ray for diagnosis.
References:
1. Miller RE, Becker GJ, Slabsugh RD: Detection of pneumoperitoneum, Optimum body position and respiratory phase; AJR 1980, 135:487.
2. Hugh TB, Perforated peptic ulcers in Maingot’s abdominal operations, Seymour I. Schwartz and Harold Ellis, 9th edition, vol-1, Appleton & Lange, 1990, p.633
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





