IJCRR - 5(18), September, 2013
Pages: 60-64
Date of Publication: 25-Sep-2013
Print Article
Download XML Download PDF
A STUDY ON THE ASSOCIATION OF HYPERTELORISM AND POSTERIORLY PLACED PINNA IN CHILDREN WITH CONGENITAL ACYANOTIC HEART DISEASES
Author: Sumi Ghorai, Swapan Bhattacharya
Category: Healthcare
Abstract:Objective: To diagnose undetected cases of asymptomatic congenital acyanotic heart disease by measuring intercanthal distance (ICD) and angle of ear inclination (AEI). Methods: A comparative study was conducted over a period of 2011-2012 in the Department of Paediatric Medicine, Medical College Hospital, Kolkata. 100 patients (Cases: 50 patients with congenital acyanotic heart disease. Control: 50 patients without it) of age group 3 months to 12 years were examined clinically. Echocardiography was done. Intercanthal distance was measured by Vernier's sliding caliper and angle of ear inclination by photogrametry. Results: Among 50 cases, 7(14%) male and 14(28%) female patients had hypertelorism, 10(20%) male and 16(32%) female patients had posteriorly rotated pinna. Among 50 controls, 4(8%) male, and 6(12%) female patients had hypertelorism and 2(4%) male, and 6(12%) female patients had posteriorly rotated pinna. In both the group female patients had higher incidence. Conclusion: Every child with hypertelorism and obliquely placed pinna should be properly screened for congenital acyanotic heart disease to decrease the morbidity.
Keywords: Pinna, hypertelorism, Congenital acyanotic heart disease.
Full Text:
INTRODUCTION
Craniofacial anthropometry has mostly been used as a descriptive tool and has helped clinicians in the description, diagnosis and surgical treatment of abnormal skeletal and facial patterns. It is especially useful in medical genetics because many of the syndromes present at birth-such as Apert, Down, Turner etc.-involve the head region, so it can assist clinicians to objectively describe what they are seeing”.1 The diagnosis of many dysmorphic syndromes is based not only on advanced cytogenetic and molecular techniques, but also on recognition of subtle morphological anomalies in craniofacial region. Dysmorphic characters are usually reported by clinicians in descriptive terms such as “wide set eyes”,”broad nose”,”large mouth” and “posteriorly placed ear”. However, such description is subjective. Measurements taken from a patient can be compared with the values obtained in normal population and deviations from the normative values can be evaluated.2 The present study was conducted not only to compare the intercanthal distance of the controls without congenital acyanotic heart disease to cases with it but also to acquire knowledge about position of the pinna or angle of ear inclination in cases with congenital acyanotic heart disease and correlate it with the controls. In normal individual the intercanthal distance is about 2 cm to 3.6 cm and angle of ear inclination is approximately 7-120. Deviation from the normal can be indicative of congenital anomalies.
MATERIALS AND METHOD
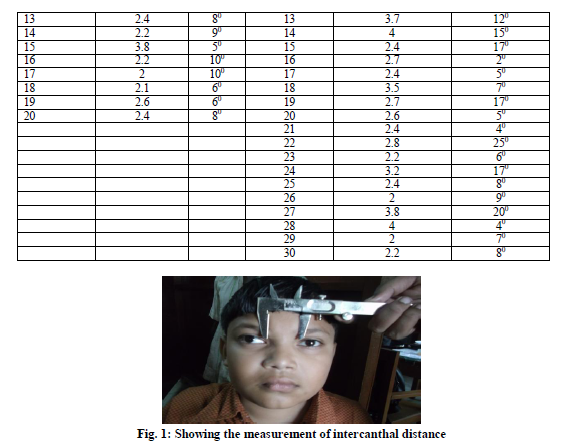
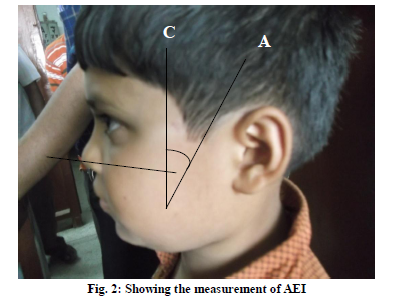
The study was conducted on 100 patients of age group 3 months to 12 years attending the outpatient department and or, admitted in the department of Paediatric Medicine, Medical College, Kolkata over a period of 2011-2012. Thorough clinical examination of cardiovascular system was done. Echocardiography of the children were performed to confirm the diagnosis. Clinical examinations were done in presence of paediatricians and echocardiographies were done. The intercanthal distance was measured by vernier’s sliding caliper taking into account the error if any, in the instrument (Fig. 1). Profile photograph of the left side of the face of all children was taken including the entire helical rim of left ear, while keeping the head in the Frankfurt Horizontal (FH) plane. The angle of ear inclination (AEI) was directly measured on the photograph fixed on a large white paper sheet. The angle subtended between longitudinal axis(AB) of ear. It was determine as per technique given by Farkas LG3; the line joining highest point on superior aspect of outer rim of helix to the most lowest point on the inferior border of ear lobule and vertical plane(BC) of the head/face represented by a perpendicular drawn on FH plane (FH plane: line extending from the lower border of the left orbit to the upper margin of the external auditory meatus, provided head is held erect and eyes looking straight forward) was considered as angle of ear inclination(AEI)(Fig. 2). The angle was measured with the help of a protractor upto the accuracy of one degree. Each measurement was taken twice by the same examiner. If there is large difference between the initial two measurements a third reading was taken. Among the three measurements the two nearer values were used.
RESULTS
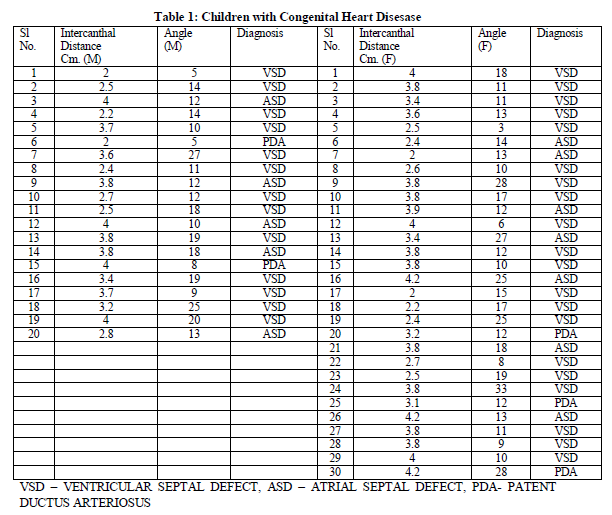
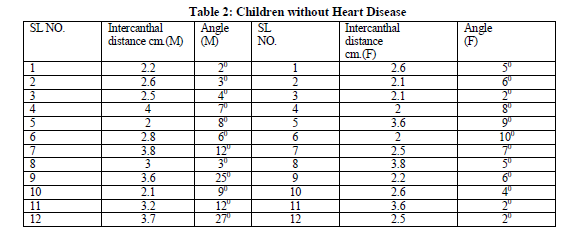
The study was conducted on 100 patients, 50 cases and 50 controls. Out of those 20 were male and 30 were female in both the group. The age range was 3months to 12 years. In this study 7(14%) male and 14(28%) female patients had hypertelorism and 10(20%) male and 16(32%) female patients had posteriorly rotated pinna among the 50 cases with Congenital acyanotic heart disease (Table1). Whereas, 4(8%) male,10(12%) female patients had hypertelorism and 2(4%) male,6(12%) female patients had posteriorly rotated pinna out of 50 patients without Congenital acyanotic heart disease(table 2).
DISCUSSION
The values for AEI reported by Farkas LG4 ranged between 6.3°-35.6° (mean 20°) in normal girls and 9.3°-31.2° (mean 21°) in boys. However, he had not examined the heart and has therefore, not commented on any co-existing cardiac abnormality.
Walia BNS et al5 reported that 18 of the 20 subjects with congenital heart disease having angle of ear inclination more than 12° on photographic measurement, and concluded the mean AEI in heart defects was more than two times as compared to children who had normal ears and normal hearts. In our study 26(52%) of 50 patients with congenital acyanotic heart disease had AEI more than 12°. Of these 26 subjects 10(38.46%) were male,16(61.54%) were female.
Nair S et al6 reported one case of congenital acyanotic heart disease - Ventricular septal defect(VSD), Atrial septal defect(ASD),Patent ductus arteriosus( PDA) with pulmonary hypertension with hypertelorism, low set dysmorphic ears and other facial dysmorphism.
In our study 7(14%) male and 14(28%) female patients with heart disease had hypertelorism.
Noonan’s syndrome is one of the multiple congenital anomaly syndrome which is related with hypertelorism, cardiac defect and many other anomalies as per study of Bertola DR et al7. Our study did show co-relation between heart disease and hypertelorism, as there are 21 subjects who had increased intercanthal distance out of 50 patients with acyanotic heart disease. From the above discussion it can be said that, hypertelorism and obliquely placed pinna is associated with congenital acyanotic heart diseases. During embryologic development, external ear appears in the region around the first pharyngeal groove in the 2nd month and interventricular septum also develops at about the same time. It is possible that the same agent/stimulus acting at this period distorts the development of both the regions simultaneously8.
Neural crest cells are essential for formation of much of the craniofacial region and they also contribute to the conotruncal endocardial cushions, which septate the outflow tract of the heart into pulmonary and aortic channels. So, this might be reason for infants to have cardiac abnormalities with craniofacial defects.9
CONCLUSION
From the above discussion it has been proved that there is certainly a relationship between hypertelorism and congenital acyanotic heart disease. Though, of 50 patients without heart disease 4(8%) male,6(12%) female patients had hypertelorism and 2(4%) male,6(12%) female patients had posteriorly rotated pinna ,that is far less common than in subjects with congenital acyanotic heart disease.
Our data suggest that any child whose pinna appears obliquely placed and eyes look apart on clinical examination should be carefully investigated for coexistence of unrecognized congenital cardiac anomalies.
ACKNOWLEDGEMENT
The authors of this article gratefully acknowledge the inspiration and help received from the scholars whose articles have been cited in the reference section. The authors pay their gratitude to authors/editors/publishers of all those articles/journals/books from where the reviews and literatures for the discussion have been collected.
References:
- Identifying fetal alcohol syndrome using computerized craniofacial anthropometry. Medical news today article. Date 27th September 2007. Available form: http://www.medicalnewstoday.com/releases/83589.php. [last cited on 13/08/2013.]
- Naglel E, Teibe U, Kapoka D. Craniofacial anthropometry in a group of healthy Latvian residents. Acta Medica Lituanica 2005;12 :47-53.
- Farkas LG. Anthropometry of Head and Face. 2nd edition, p-3-56.
- Farkas LG. Anthropometry of normal and defective ears. Clin Plast Surg 1990; 17: 213-21.
- Walia BNS, Bhalla AK, Dhawan A. Co-Existence Of Oblique Pinnae And Congenital Heart Disease. Indian Pediatrics 1994;31:559-63.
- Nair S, Varghese R, Hashim S, Scariah P. Dysmorphic features and congenital heart disease in chromosome 6q deletion. Indian Journal of Human genetics 2012;18:127-29.
- Bertola DR, Sugayama SMM, Albano LMJ, Kim CA ,Gonzalez CH. Noonan Syndrome: A Clinical And Genetic Study Of 31 Patients. Rev. Hosp. Clin. Fac. Med. S.Paulo 1999;54:147-50.
- Hamilton WJ, Mossman HW. Human Embryology. Cambridge, W. Heffer and Sons Ltd, 1972,186-88 , 289.
- Sadler TW. Langman’s Medical Embyology. 9th edition. Baltimore, Maryland, USA: Lippincott Williams and Wilkins; 2004.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





