IJCRR - 5(19), October, 2013
Pages: 126-131
Date of Publication: 19-Oct-2013
Print Article
Download XML Download PDF
DIMENSIONAL CHANGES OF TRACHEA IN SECOND AND THIRD TRIMESTER FETUSES -AN ANATOMICAL STUDY
Author: Anne Dsouza, Vrinda Hari Ankolekar, Mamatha Hosapatna, Antony sylvan Dsouza
Category: Healthcare
Abstract:Introduction: Advances in neonatal medicine have led to the early diagnosis and treatment of respiratory diseases, and the recent development of fetal airway surgery. Data on the growth of the trachea and bronchi are not readily available to the anesthesiologist and bronchoscopist in spite of the obvious clinical interest. The aim of this study was to determine the anatomical development of tracheal structures during the fetal periods and to correlate these observations with other fetal biometric parameters to estimate developmental particularities of the fetal airway. Materials and methods: The study was carried out in the department of Anatomy, on 28 human fetuses of known gestational age (GA) from spontaneous abortions or stillbirths, aged 16\?37 weeks of gestation which were categorized into second and third ( trimesters. Following parameters were noted prebifurcation length (PL), birfurcation length (BL), bifurcation-to-prebifurcation length ratio (BL/PL), Upper external transverse diameter (UD), Lower external transverse diameter (LD), Circumference (C) of trachea at the level of last tracheal cartilage. Results: The mean and standard deviations were calculated for second and third trimester and values were compared using student t-test. There was significant difference in means for PL, UD and LD between second and third trimesters. The various parameters were correlated with GA using Pearson's correlation test. SPSS version 16 was used for the statistical analysis. No significant correlation was found for LD (r=0.2, p=0.2) and for C (r=0.19, p=0.3). Conclusion: Authors conclude that the tracheal length increases significantly proportional to the GA, but not the diameter.
Keywords: trachea, prebifurcation length, bifurcation length
Full Text:
INTRODUCTION
Advances in neonatal medicine have led to the early diagnosis and treatment of respiratory diseases, and the recent development of fetal airway surgery1. Data on the growth of the trachea and bronchi are not readily available to the anesthesiologist and bronchoscopist in spite of the obvious clinical interest2. Advances in neonatal medicine have contributed to the survival of extremely preterm infants. Because of their respiratory immaturity, long-term tracheal intubation is often necessary. Practical determination of endotracheal tube size in the premature population is classically based on clinical report3,4,5,6,7. Changes in tracheal dimensions occur in a variety of conditions. For example, generalized widening is a characteristic feature of tracheobronchomegaly and tracheomalacia; generalized narrowing is seen in tracheobronchopathia osteochondroplastica and may be a feature of relapsing polychondritis8. The study of the development of the fetal trachea provides information on the functional morphology of this organ9. The aim of this study was to determine the anatomical development of tracheal structures during the fetal periods and to correlate these observations with other fetal biometric parameters to estimate developmental particularities of the fetal airway. The parameters measured in the present study will help in placement of endotracheal tube of accurate size in premature infants. These measurements should be useful in the detection of tracheal abnormalities, problems in respiratory physiology and in endotracheal intubation, endoscopy and tracheostomy.
MATERIAL AND METHODS
The study was carried out in the department of Anatomy, Kasturba Medical College, Manipal, on 28 human fetuses of known gestational age (GA) from spontaneous abortions or stillbirths, aged 16–37 weeks of gestation which were categorized into second (N=10) and third (N=18) trimesters. The specimens were immersed in 10% formalin solution. The fetuses with any external malformations were excluded from the study .The part of respiratory tract from the level of cricoid cartilage up to the hilum of lung of each foetus was resected. After clearing the soft tissues tracheal rings were visualized and the following parameters were noted using vernier calipers as shown in fig 1,
- Prebifurcation length (PL), corresponding to the distance between the superior border of the first tracheal cartilage and the inferior border of the last tracheal cartilage
b) Bifurcation length (BL), corresponding to the distance between the inferior border of the last tracheal cartilage and the tracheal bifurcation
c) Bifurcation-to-prebifurcation length ratio (BL/PL)
d) Upper external transverse diameter (UD), measured at the level of the first tracheal cartilage
e) Lower external transverse diameter (LD), measured at the level of the last tracheal cartilage.
f) Circumference (C) of trachea at the level of last tracheal cartilage.
The mean and standard deviations were calculated for second and third trimester and values were compared using student t-test. The various parameters were correlated with GA using Pearson’s correlation test. SPSS version 16 was used for the statistical analysis.
RESULTS
The present study included 10 second trimester and 18 third trimester fetuses. The mean and standard deviation of various parameters measured is shown in table 1. Student t-test was used to determine the significance between the means of second and third trimester. There was significant difference in means for PL, UD and LD between second and third trimesters.
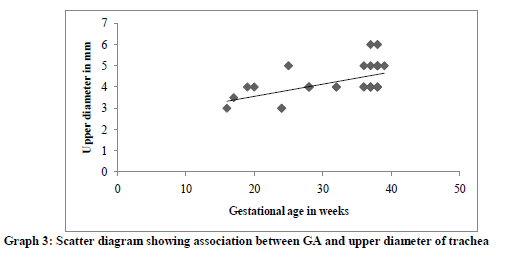
Pearson’s correlation test was done to correlate the various parameters with GA. There was a positive correlation for PL (r=0.58, p=0.001), BL (r=0.39, p=0.036) and for UD (r=0.55, p=0.002). The correlation is denoted in graphs 1, 2 and 3. No significant correlation was found for LD (r=0.2, p=0.2) and for C (r=0.19, p=0.3).
DISCUSSION
There are few studies in literature published on the anatomical measurements of the airway in pediatric populations or premature populations10, 11, 12. Tracheal dimensions undergo considerable change according to GA14. As the mid trachea is approached there is an antero-posterior flattening which yields a more elliptical section. From the mid-trachea to carina the section rounds out again and flares into right and left bronchi2. Different methods have been described to illustrate observations of fetal measurements and to estimate age-specific reference intervals for these measurements15, 16. According to Szpinda et al no significant male–female differences for any of tracheal parameters were found17. Most authors reported that both length and diameters of the trachea increased with advanced fetal age in a proportional fashion. According to Szpinda et al, the PL ranged from 8.14 ± 1.90 to 20.77 ± 0.50 mm, BL ranged from 2.23 ± 0.25 to 5.77 ± 0.76 mm, the external transverse diameters of the trachea were found to increase from 2.39 ± 0.04 to 5.20 ± 0.17 mm and from 2.42 ± 0.20 to 4.93 ± 0.08 mm for proximal and distal ends of the trachea, respectively17.A study done by Harjeeth et al showed the average length of fetal trachea was 33.07 ± 1.44mm and the average UD was 5.83 ± 1.18mm18. In the present study the PL ranged from ranged from 20.6±5.66 to 25.16±3.68 mm, BL was ranged from 3.04±0.95 to 3.66±0.97mm, UD ranged from 3.75±0.63 to 4.5±.7mm and LD ranged from 4.2±0.82m to 4.94±0.87mm, which were consistent with values obtained by Harjeeth. In the present study the length and upper diameter of trachea increased significantly in third trimester. Whereas the tracheal diameters did not increased significantly with gestational age. Few studies have been published on the anatomical measurements of the airway in either pediatric population or premature population19, 20.
CONCLUSION
Authors conclude that the tracheal length increases significantly proportional to the GA, but not the diameter. Generalized widening is a characteristic feature of tracheobronchomegaly and tracheomalacia; generalized narrowing is seen in tracheobronchopathia osteochondroplastica. Hence the study of the development of the fetal trachea provides information on the functional morphology of this organ.
ACKNOWLEDGEMENT
The authors sincerely thank the post graduate students and non-teaching staff of Anatomy, KMC Manipal for their valuable contribution to the work.



References:
- Wagner W, Harrison MR Fetal operations in the head and neck area: current state. Head Neck 2002; 24:482–90.
- Ralph O. Butz, Jr. Length and cross-section growth patterns in the human trachea. Pediatrics 1968;42:336
- Ratner I, Whitfield J: Acquired subglottic stenosis in the very-low-birthweight infant. Am J Dis Child 1983; 137:40–3
- Laing IA, Cowan DL, Ballantine GM, Hume R: Prevention of subglottic stenosis in neonatal ventilation. Int J Pediatr Otorhinolaryngol 1986; 11:61–6
- Contensin P, Narcy P: Size of endotracheal tube and neonatal acquired subglottic stenosis. Study Group for Neonatology and Pediatric Emergencies in the Parisian Area. Arch Otolaryngol Head Neck Surg 1993; 119:815–9
- Kattwinkel J, Niermeyer S, Nadkarni V, Tibballs J, Phillips B, Zideman D,Van Reempt P, Osmond M: Resuscitation of the newly born infant: An advisory statement from the Pediatric Working Group of the International Liaison Committee on Resuscitation. Resuscitation 1999; 40:71–88
- Niermeyer S, Kattwinkel J, Van Reempts P, Nadkarni V, Phillips B, Zideman D, Azzopardi D, Berg R, Boyle D, Boyle R, Burchfield D, Carlo W, Chameides L, Denson S, Fallat M, Gerardi M, Gunn A, Hazinski MF, Keenan W, Knaebel S, Milner A, Perlman J, Saugstad OD, Schleien C, Solimano A, Speer M, Toce S, Wiswell T, Zaritski A: International guidelines for neonatal resuscitation: An excerpt from the guidelines 2000 for cardiopulmonary resuscitation and emergency cardiovascular care: International consensus on science. Pediatrics 2000;106:e29
- Breatnach E, Abbott GC, Fraser RG. Dimensions of the Normal Human Trachea. AJR 1984;141:903-906
- Montgomery PQ, Stafford ND, Stolinskit C. Ultrastructure of human fetal trachea. A morphological study of the luminal and glandular epithelia at the mid-trimester. J. Anat. 1990; 173:43-59
- Tucker GF, Tucker JA, Vidic B: Anatomy and development of the cricoid: Serial section whole organ study of perinatal larynges. Ann Otol Rhinol Laryngol. 1977; 86:766–9
- Eckel HE, Koebke J, Sittel C, Sprinzl GM, and Pototschnig C, Stennert E: Morphology of the human larynx during the first five years of life studied on whole organ serial sections. Ann Otol Rhinol Laryngol 1999; 108:232–7
- Wilson TG: Some observations on the anatomy of the infantile larynx. Acta Otolaryngol 1953; 43:95–9
- Fearon B, Whalen JS: Tracheal dimensions in the living infant (preliminary report). Ann Otol Rhinol Laryngol 1967; 76:965–74
- Gnscom T, B. WohI ME. Dimensions of the Growing Trachea Related to Age and Gender. AJR 1986;146:233-237
- Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. 1992; 11:1305–1319.
- Royston P, Wright EM. How to construct ‘normal ranges’ for fetal variables.Ultrasound Obstet Gynecol. 1998; 11:30–38.
- Szpinda M, Daroszewski M, Wosniak A, Szpinda A, Kierzenkowska CM. Tracheal dimensions in human fetuses: an anatomical, digital and statistical study. Surg Radiol Anat (2012) 34:317–323
- Harjeet J, Sahni D, Batra YK, Rajeev S (2008) Anatomical dimensions of trachea, main bronchi, subcarinal and bronchial angles in fetuses measured ex vivo. Paediatr Anaesth 18:1029–1034
- Tucker GF, Tucker JA, Vidic B: Anatomy and development of the cricoid: Serial section whole organ study of perinatal larynges. Ann Otol Rhinol Laryngol 1977; 86:766–9
- Eckel HE, Koebke J, Sittel C, Sprinzl GM, Pototschnig C, and Stennert E Morphology of the human larynx during the first five years of life studied on whole organ serial sections. Ann Otol Rhinol Laryngol 1999; 108:232–7
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





