IJCRR - 5(19), October, 2013
Pages: 88-90
Date of Publication: 19-Oct-2013
Print Article
Download XML Download PDF
TRAUMATIC RECTAL PERFORATION MANAGED BY SIMPLE CLOSURE WITHOUT COLOSTOMY
Author: A. Saravanan, G. Ganesan, K. Vivekananda Subramania Nathan
Category: Healthcare
Abstract:Generally traumatic rectal perforations are managed by doing diverting colostomy along with simple closure. Here we are reporting a case of traumatic rectal perforation which is managed by doing simple closure alone without diverting colostomy. About 95% of rectal injuries are due to penetrating injuries. Rectal injuries due to blunt trauma are rare but have more disastrous outcome .Extraperitoneal perforations of the lower part of the rectum are usually due to blunt injury and access to the area of perforation and closure is extremely tough. Hence extraperitoneal perforation has a bad prognosis and always requires diverting colostomy. Large intraperitoneal perforations of the upper part of the rectum involving the anterior wall are commonly associated with concomitant injuries and always require diverting colostomy. Patients presenting late are usually associated with severe peritoneal contamination and have bad prognosis and always require diverting colostomy. But small intraperitoneal perforations of the posterior wall of the upper part of the rectum are not commonly associated with concomitant injuries like in the patient reported below and do not require diverting colostomy, if the patient presents early without serious peritoneal contamination.
Keywords: Rectal perforations, simple closure, diverting colostomy.
Full Text:
INTRODUCTION
Rectal perforation is generally managed by doing diverting colostomy along with closure of perforation [1-9]. But so far there have been very few reports of managing rectal perforation by doing only simple closure without colostomy. Hence a case of rectal perforation managed by doing only simple closure without colostomy is reported here.
CASE REPORT
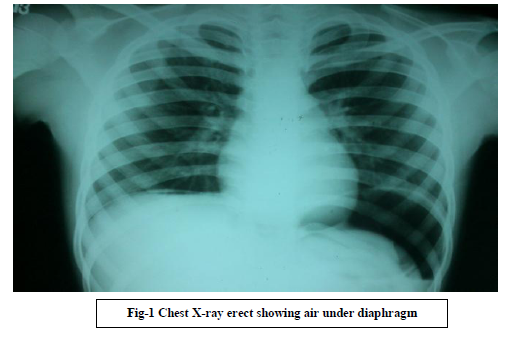
A thirteen year old boy had an accidental penetrating injury to his rectum by a wooden stick and presented within 18 hours of his injury with signs of generalized peritonitis, X-ray chest showed pneumoperitoneum (Fig-1).
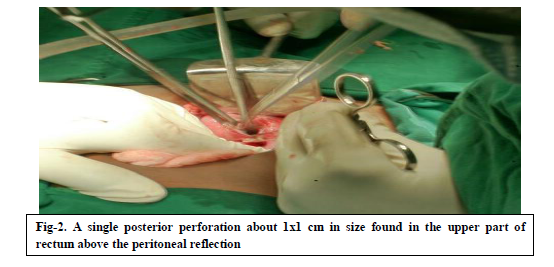
Laparotomy was done immediately and 250ml of pus was found in the peritoneal cavity. A single small 1x1cm intraperitoneal perforation was found in the posterior wall of upper part of rectum (Fig-2) and was closed with single layer of interrupted 3.0 silk. The patient recovered uneventfully.
DISCUSSION
Perforation of the lower part of the rectum (extraperitoneal perforation) is extremely difficult to access by laparotomy and hence closure is extremely tough. But perforation in this patient was intraperitoneal lying at the upper most part of rectum and closure could be done easily. In addition, our patient presented within 18 hours of injury and there was no faecal contamination of peritoneal cavity. Hence a diverting colostomy was not done.
Patients with rectal perforation presenting early have good prognosis. But patients presenting late
are usually associated with very severe and serious peritoneal contamination and have bad prognosis [9] and always require diverting colostomy.
About 95% of rectal injuries are due to penetrating injuries [5]. Rectal injuries due to blunt trauma are rare [5, 8] but have more disastrous outcome [5]. Extraperitoneal perforations occurring in the lower part of the rectum are usually due to blunt injury [5, 8, 10], commonly associated with fracture of pelvic bones [5, 8, 10] and sepsis of perirectal tissues [5, 10] and pelvic abscess [10]. Access to the area of perforation and closure is extremely tough while doing laparotomy. Hence extraperitoneal perforation has a bad prognosis and always requires diverting colostomy [5].
Large intraperitoneal perforations of anterior wall of the upper part of the rectum are commonly associated with concomitant injuries to urinary bladder [ 2], seminal vesicles[3], uterus,small bowel mesentery [ 11], sigmoid mesocolon [3,11] etc. and sometimes even evisceration of the small bowel [4,12] and always require diverting colostomy.
CONCLUSION
Small intraperitoneal perforations of the posterior wall of the upper part of the rectum are not commonly associated with concomitant injuries like in this patient and do not require diverting colostomy, if the patient presents early without serious peritoneal contamination.
But all extraperitoneal perforations, large intraperitoneal perforations of the anterior wall associated with concomitant injuries and patients presenting late with very serious peritoneal contamination always require diverting colostomy along with closure of the perforation.
References:
- Emil Mammadov, Altan Alim, Mehmet Elicevik and Sinan Celayir., Self-induced penetrating rectal perforation by foreign body: an unusual event in childhood., Annals of Pediatric Surgery 2011, 7:25–26.
- Mahmoud Aghaei Afshar, Foroogh Mangeli and Akram Nakheai., A Rare Case of Anorectal Injury with Ruptured Bladder and Rectum but Normal Anal Sphincter.,J Clin Case Rep 2012, 2:14.
- Major D S Jackson., Accidental Impalement Injuries of the Intraperitoneal Rectum caused by the Barrel of the Self Loading Rifle., J R Army Med Corps 1985; 131: 164-166.
- Neil R Price, S V Soundappan, Anthony L Sparnon and Danny T Cass., Swimming pool filter-induced transrectal evisceration in children: Australian experience., MJA?.Volume 192 Number 9. 3 May 2010; 534-536.
- Isaac Chun-Jen Chen, Hsin-Chin Shih, Yi-Szu Wen., Extraperitoneal Rectal Perforation without Perineal Wound or Pelvic Fracture., J Chin Med Assoc 2004;67:637-639.
- Ayeed Al-Qahtani ; Abdulkarim El-Wassabi ; Abdulrahman Al-Bassam .., Mercury-In-Glass Thermometer As A Cause Of Neonatal Rectal Perforations: A Report Of Three Cases And Review Of The Literature…, Annals of Saudi Medicine, Vol 21, Nos 1-2, 2001
- Charles G. Roland, Arnold G. Rogers.., Rectal Perforations After Enema Administration, canad.M.A.J.nov.15,1959, vol.81.
- Rachel M. Gomes, Jayesh Kudchadkar,Edwin Araujo, Trupti Gundawar,Anorectal avulsion: report of a rare case of rectal injury, Annals of Gastroenterology (2013) 26, 1
- Aditya Yelikar ,Tejinder Singh Chhabda , Pravin Suryawanshi …,Laparoscopic Management of Rectal Perforation Secondary To Self Induced Foreign Body – A Rare Case Report …,IJSR - International Journal Of Scientific Research Volume :2 Issue :1 Jan 2013 .ISSN No 2277 – 8179.
- J F Nolan., Delayed presentation of rectal perforation. , Journal of the Royal Society of Medicine Volume 83 November 1990; 744-745.
- Karger B, Teige K, Bajanowski T. Bizarre impalement fatalities—where is the implement? J Forensic Sci 2002;47(2):389–391.
- Naima Zamir, Ahmed Sharif, M.Aqil Soomro, Soofia Ahmed And Jamshed Akhtar, Rectal Perforation in Children, Journal of The College of Physicians and Surgeons Pakistan 2008, Vol. 18 (1): 66-67.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





