IJCRR - 5(19), October, 2013
Pages: 66-68
Date of Publication: 19-Oct-2013
Print Article
Download XML Download PDF
DISASTROUS REACTION TO METHYLENE BLUE DYE - A CASE REPORT
Author: K. Natarajan, N. Murugesan
Category: Healthcare
Abstract:Methylene blue is used as a diagnostic and therapeutic agent in humans. Adverse reaction to the dye is very rare. But when adverse reaction occurs it can be very severe and dangerous. The reaction may be local or generalized and sometimes life threatening and can be even fatal. This should be kept in mind to avoid or minimize the severe reactions to the dye. We hereby present a female patient who developed severe chemical peritonitis with small bowel perforations to the methylene blue dye in the course of investigation for primary infertility.
Keywords: Methylene blue, Chemical peritonitis, Ileal perforation
Full Text:
INTRODUCTION
Methylene blue is a versatile dye which is used in a variety of situations from diagnosis to therapy, across all branches of medicine. It is used in the investigations of sinuses, fistula, sentinel node localization in malignancy, normal and abnormal tissue identification (tattooing of colonic mucosa during colonoscopy) and patency of Fallopian tubes. Gynecologists routinely use methylene blue dye solution to test the patency of Fallopian tubes in the course of investigations for infertility. Reactions to the dye are very rare. But when it occurs it can be very serious and can lead to major complications like chemical peritonitis1,2,3, general skin reactions, tissue necrosis4,5, methemogobinemia6,7, anaphylaxis8, pulmonary edema09,10 etc.
CASE REPORT
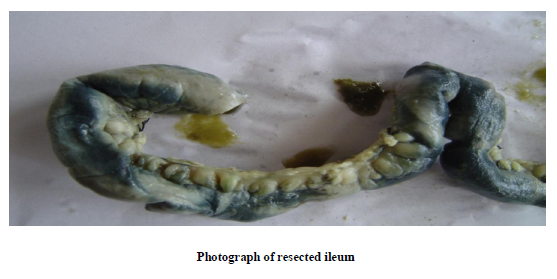
A 30 year old patient underwent diagnostic laparoscopy and tube patency test using 0.5% sterile methylene blue dye solution. The whole procedure was uneventful. She recovered from the anaesthesia completely and started taking oral fluids after 6 hours. She developed lower abdominal pain after 24 hours which was constant and not associated with any vomiting. On examination she had mild diffuse tenderness in the lower abdomen with no rebound tenderness. Bowel sounds were present. She was started on IV fluids and antibiotics and kept nil oral. She continued to have abdominal pain and on the fourth day developed severe abdominal pain with signs of peritonitis. Immediately she underwent emergency laparotomy. At laparotomy the peritoneal cavity was found to have turbid fluid. The terminal ileum was stained in many parts with methylene blue and there were four perforations in the areas of blue staining. The terminal part of the ileum was thickened, white and found not viable. The terminal ileum with the perforations was resected and end to end anastomosis was done. She recovered slowly and was started on oral fluids after flatus was passed. She developed a small bowel fistula in the lower part of the abdominal wound on the 20th day. She was treated conservatively with NPO and IV fluids. Ultra sound examination of the abdomen did not show
any intra peritoneal collection or any other abnormality. The fistula closed spontaneously within a week. She was discharged home afterwards. Histopathological examination of the resected bowel showed severe diffuse inflammation of the small bowel with multiple perforations.
In the course of the next 6 months she had intermittent discharge of small bowel contents from the same area of previous small bowel fistula. Each time it closed spontaneously.
She underwent Ultrasound examination of the abdomen which did not reveal any abnormality. CT Abdomen also was normal. Fistulogram showed filling of the small bowel with the contrast. Large bowel was not filled with the contrast.
After these investigations she underwent an elective Laparotomy under GA. At laparotomy stricture of the terminal ileum beyond the fistulous opening was found. That part was resected and ileo caecal anastomosis was performed. The post operative period was uneventful.
DISCUSSION
Literature is very limited due to the rarity of the adverse reaction to the dye and only a few references are available. Various types of reaction to methylene blue dye like anaphylaxis8, methemoglobinemia6,7, pulmonary oedema09,10, chemical peritonitis1,2,3 or local skin reactions4,5 have been described. The patient in this report developed severe chemical peritonitis with multiple perforations of the small bowel. Formation of intraperitoneal adhesions in rats is reported in experimental studies11. To prevent adverse reactions to the dye, O’Sullivan advises the use of very dilute solution of the dye(1 ml of 1% methylene blue dye diluted in 100 ml of sterile saline). Aspiration of the dye from the peritoneal cavity and steroid wash to the areas of contact with the dye after completing the procedure might also help.
CONCLUSION
Adverse reaction to methylene blue dye is very rare. The reaction may be local at the site of application or general. The physician using the dye must take appropriate preventive steps like using very dilute solution, aspirating the dye after usage and giving steroid lavage. When adverse reaction occurs this should be treated promptly. The adverse reactions, the preventive measures and treatment are to be kept in mind whenever this dye is used.
References:
- Nolan DG. Inflammatory peritonitis with ascites after methylene blue dye
chromopertubation during diagnostic laparoscopy. J Am Assoc Gynecol
Laparosc 1995; 2: 483–485.
- Macia M, Gallego E, Garcia-Cobaleda I et al. Methylene blue as a cause of chemical peritonitis in a patient on peritoneal dialysis. Clin Nephrol 1995; 43: 136–137
- O’Sullivan JC. Female sterility produced by investigation, Br. Med. J.; Vol 4 ISS Nov. 24,1973, P490
- M Salhab, W Al sarakbi and K Mokbel Skin and fat necrosis of the breast following methylene blue dye injection for sentinel node biopsy in a patient with breast cancer International Seminars in Surgical Oncology 2005, 2:26 doi:10.1186/1477-7800-2-26
- Stradling B, Aranha G, Gabram S. Adverse skin lesions after methylene blue injections for sentinel node localization. Am J Surg. 2002 Oct; 184(4):350-2
- Mhaskar R, Mhaskar AM Methemoglobinemia following chromopertubation in treated pelvic tuberculosis. Int J Gynaecol Obstet. 2002 Apr;77(1):41-2. PMID:11929658 [PubMed - indexed for MEDLINE]
- Bilgin H, Ozcan B, Bilgin T. Methemoglobinemia induced by methylene blue pertubation during laparoscopy.Acta Anaesthesiol Scand. 1998 May;42(5):594-5.PMID:9605379 [PubMed - indexed for MEDLINE]
- Rzymski P, Wozniak J, Opala T, Wilczak M, Sajdak S. Anaphylactic reaction to methylene blue dye after laparoscopic chromopertubation. Int J Gynaecol Obstet. 2003 Apr; 81(1):71-2.
- Teknos D, Ramcharan A, Oluwole SF Pulmonary edema associated with methylene blue dye administration during sentinel lymph node biopsy..J Natl Med Assoc. 2008 Dec;100(12):1483-4.PMID:19110921 [PubMed - indexed for MEDLINE]
- Millo T, Misra R, Girdhar S, Rautji R, Lalwani S, Dogra TD. Fatal pulmonary oedema following laparoscopic chromopertubation. Natl Med J India. 2006 Mar-Apr;19(2):78-9. PMID: 16756195 [PubMed - indexed for Medline]
- Gul A, Kotan C, Dilek I, Gul T, Tas A, Berktas M, Effects of methylene blue, indigo carmine solution and autologous erythrocyte suspension on formation of adhesions after injection into rats. Reprod Fertil. 2000 Nov;120(2):225-9
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





