IJCRR - 9(4), February, 2017
Pages: 21-25
Date of Publication: 20-Feb-2017
Print Article
Download XML Download PDF
Hemorrhagic risks associated with dental procedure in a rare case of Type II Sturge weber syndrome
Author: Ashwini Nerkar1, Rajeev Gadgil2, Ajay Bhoosreddy3, Karan Shah4
Category: Healthcare
Abstract:Aim: Sturge weber syndrome (SWS) is a sporadic congenital neurocutaneous disorder. It belongs to phakomatoses group of disorders. It is basically combinations of manifestations such as port-wine stains (PWS) of the face, ipsilateral leptomeningeal angioma (cerebral malformations and tumours), glaucoma, seizures and mental retardation. Sturge weber syndrome type II have no evidence of brain involvement though it shows a vascular malformation on the face and the possibility of glaucoma. We hereby delineate a case of a female, reported with PWS and diagnosed as Type II Sturge weber syndrome.
Case Report: We reported a case of a 35-year-old female who had a diffused swelling on the right maxillary region corresponding to the distribution of the cutaneous port-wine stain and glaucoma of the right eye. Positive manifestations with respect to skin, eyes and oral cavity along with negative radiographic findings, we arrived to the diagnosis of Type II Sturge weber syndrome.
Discussion: Differential diagnosis of SWS includes Rendu Osler Weber syndrome, Von Hippel Lindau Disease and Maffucci Syndrome. Diagnosis is made only on the basis of clinical and imaging features.
Conclusion: Dental procedures are associated with increased possibility of hemorrhage in sturge weber syndrome. Thus, doing treatment in such patients is a difficult task for oral health care practitioners. Therefore the intent of the presented case is to keep in background a clinical scenario of similar pattern, if observed, will need to be diagnosed with utmost caution prior to any dental procedure.
Keywords: Encephalotrigeminal angiomatosis, Ocular manifestations, Oral manifestations, Sturge weber syndrome, Vascular lesions
Full Text:
INTRODUCTION
Sturge weber syndrome (SWS), also known as, meningofacial angiomatosis[1], encephalotrigeminal angiomatosis [2] and encephalotrigeminal angiomyomatosis [3] is congenital and non-familial in its origin [4]. It belongs to syndromes of phakomatoses disorders (mother-spot diseases) [4].It is one of the Systemic syndromes of Phakomatoses pigmentovascularis (PPV) [5] and is also categorized into neurocutaneous disorders[6].In 1860 Schirmer and in 1879 Sturge associated dermatological and ophthalmic manifestations to this neurologic condition ,which was later on accompanied by radiological alterations given by Weber.[7] The increase in the formulation of mutant Gaq protein is due to a somatic activating mutation in guanine nucleotide-binding protein alpha-q (GNAQ).This process is found to be affiliated with SWS [8].It is typically a static lesion but few cases with progressing lesions have been reported [9]. Estimated frequency is of 1 per 50,000 live births [10]. SWS is characterized by the presence of leptomeningeal angiomas , PWS (sharply demarcated vascular lesions that occur unilaterally along the dermatomes supplied by first two divisions of trigeminal nerve), along with ocular disorders, CNS involvement and oral involvement[11].Manifestation of the syndrome is due to endurant dysfunction of embryonal vascular system [12] which develops during the 6th week of embryonic life[13].
Presence of only two of the positive findings i.e. presence of facial angiomas , ocular involvement such as glaucoma, which may or may not be present, suggests diagnosis of Type II SWS. Complete absence of CNS involvement is a peculiar finding of type II SWS[14]. Manifestations such as ipsilateral angiomatosis of lips (causing macrochelia ) can be seen. Intraorally, gingival lesion which can be present as vascular hyperplasia or massive hemangiomatous proliferation . Also, pyogenic granulomas may be seen. Unilateral angiomatosis of buccal mucosa, palate, and floor of the mouth is seen on the affected side. Ipsilateral hypertrophy of alveolus, premature eruption, or delayed eruption and malocclusion are the other abnormalities reported till date[15]. Owing to its occasional incidence and a wide spectrum of exemplifications in its manifestations (skin +brain +eyes +oral cavity) we report a case of a female, showing idiosyncratic illustrations of this syndrome.
CASE-REPORT
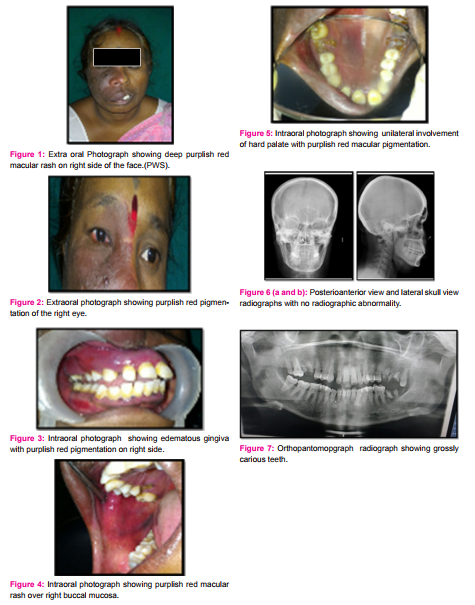
A 35 year old female reported with a chief complaint of pain and swelling on right mid-face region and presented with pigmentation in the same region, which was static in size since birth. However, with increase in the age, apparent increase in the intensity of colour, from light pink to deep purplish red was reported. Past medical history was negative with respect to any systemic problem, seizure episodes, any drug intake, trauma or abnormality during pregnancy and delivery. No relevant family history was reported. On extraoral examination a maculo-papular area of deep purplish –red pigmentation was noticed over right middle third of face which was unilateral and not crossing the midline.The rash was extending over the supraorbital region, infra-orbital region including bridge of the nose, malar region of cheek and the supralabial region along with a gross enlargement of right half of the upper lip suggestive of macrochelia [Fig 1]. Patient didn’t report any bleeding, burning sensation, numbness or parasthesia in the pigmented or surrounding areas. Examination of the right eye revealed a visual acuity of no light perception, conjunctival chemosis, episcleral haemangioma with raised intraocular pressure suggestive of glaucoma.[Fig 2]
On palpation, absence of bruit or pulsation was noticed .An intraoral examination revealed erythematous, swollen and edematous gingiva involving the right maxillary arch, which was tender on palpation and soft in consistency and restricted within the midline.[Fig 3]. Similar macular purplish red patch was seen involving the right side of the buccal mucosa [Fig 4] and on hard palate extending to the midline.[Fig 6]. Patient’s oral hygiene was poor and showed chronic generalized periodontitis, spacing with maxillary anteriors and prognathic maxilla.[Fig 3].
A Lateral skull and PA radiograph was advised to find out presence of any tram track gyral calcifications but did not reveal any such changes.[Fig 6 a&b ]. The haemogram of the patient was well within normal limits. Based upon history and clinical appearance a final diagnosis of type II SWS was given. Patient along with her family was educated and made aware about the condition and the possible complications that could arise during the necessary dental procedures. She was prescribed with antibiotics and analgesics course of 5days and advised for oral prophylaxis and extraction with all grossly carious teeth[Fig 7] followed by replacement with fixed prosthesis.
DISCUSSION
According to National Institute of Neurological Disorders and Stroke, SWS is a neurological disorder. It is characterized by a congenital facial birthmark, known as a capillary malformation and other neurological abnormalities. The other symptoms include eye and internal organ irregularities which vary in degree [15]. It has no racial or sex predilection [16].
The most apparent sign of SWS is a birthmark or PWS on the face. The PWS is due to an overabundance of capillaries just beneath the surface of the involved areas. When the port wine stain covers the eye and forehead region of the face, SWS should be considered. In rare instances, SWS is present even in the absence of the PWS [17].
SWS can be cited as comprehensive only when both CNS and facial angiomas are present and is considered to be fragmentary when only one area is affected without the other .It can be classified as complete and incomplete depending on presence of facial and leptomeningeal angioma [18]. Roach developed a scale for classification which is as follows [19].
Type I - Both facial and leptomeningeal angiomas; may have glaucoma
Type II - Facial angioma alone (no CNS involvement); may have glaucoma
Type III - Isolated leptomeningeal angioma; usually no glaucoma.
The oral manifestations include ipsilateral PWS of oral mucosa along with the hypervascular changes. Angiomatous lesions of gingiva which can vary from slight vascular hyperplasia to hemangiomatous proliferation. It is characterized by increase in the vascular component and gingival hemorrhage at minimal trauma [6,19,20].Gingival hyperplasia can also be attributed to anticonvulsant medication and secondary to poor oral hygiene in mentally retarded patients. Macroglossia and maxillary bone hypertrophy have also been reported in a few cases [21].
The ocular complications manifests as glaucoma, vascular malformations conjunctiva, episclera, choroid and retina. This may produce a localized or diffuse pinkish discoloration of the bulbar conjunctiva especially in the limbus zone. [7].
Tram track calcification caused by in opposing gyri, ipsilateral calvarial thickening and enlargement of the paranasal sinuses and mastoid may be visible in skull films. Higher imaging modalities like CT for calcification and MRI for brain assessment can also be used. MRI is the current gold standard for diagnosis of this disease especially in infants [23] .
Differential diagnosis of SWS includes Rendu Osler Weber syndrome, Von Hippel Lindau Disease and Maffucci Syndrome. Diagnosis is made only on the basis of clinical and imaging features [24].
Hereditary hemorrhagic telangiectasia (HHT) or Rendu Osler Weber Syndrome along with positive family history is characterized by the presence Nosebleeds (epistaxis), mucocutaneous telangiectases and visceral arteriovenous malformation (AVM). AVM’s may be pulmonary, cerebral, hepatic, spinal, gastrointestinal and pancreatic. The clinical diagnosis of HHT is considered definite, possible or suspected and unlikely, which depends on the number of findings present[25].
Von Hippel–Lindau disease (VHL) is an autosomal dominantly inherited disorder predispose to the development of a variety of tumours (most commonly retinal and central nervous system haemangioblastomas, clear cell renal carcinoma and phaeochromocytomas). Visceral cysts (renal, pancreatic and epididymal) are common but rarely compromise organ function. Less frequent tumours include adrenal and extra-adrenal pheochromocytomas , non-functioning pancreatic endocrine cancers, endolymphatic sac tumours and occasionally, head and neck paragangliomas [26].
Maffucci syndrome is characterized by benign enlargements of cartilage (enchondromas); bone deformities; and dark, irregularly shaped hemangiomas. There is a tendency for malignant transformation of enchondromas into chondrosarcomas or of hemangiomas into vascular sarcomas. Patients with Maffucci syndrome also are susceptible to the development of other malignant lesions such as glioma [27].
Table no 1. Demonstrates classical clinical manifestations of SWS and of those present in our case. Our patient exhibited characteristic clinical manifestations of Type II SWS including PWS and oral manifestations.
Table 1 POSITIVE MANIFESTATIONS IN THE PRESENT CASE OF SWS
|
Sr.No
|
Manifestations seen in SWS
|
Present case findings
|
|
1
|
EPILEPSY
|
-
|
|
2
|
PORT WINE STAIN
|
+
|
|
3
|
ABNORMAL RADIOGRAHIC FINDINGS
|
-
|
|
4
|
MENTAL RETARDATION
|
-
|
|
5
|
ORAL MANIFESTATIONS
|
+
|
|
6
|
HEMIPARESIS
|
-
|
|
7
|
OCCULAR MANIFESTATIONS
|
+
|
Treatment and prognosis of SWS depends on the extent of involvement. PWS can cause severe psychological trauma to the patients and hamper their personality development. PWS can be improved by dermabrasion, tattooing and flash lamp pulse dyed lasers. Various treatment modalities like sclerotherapy, cryotherapy, laser and surgical excision have been tried with varying degrees of success to surmount intraoral lesions [28].
Dental management should be mostly stressed on preventive measures. Patients should be educated, motivated and complied to follow a strict oral hygiene regimen to prevent dental caries and secondary gingival inflammatory enlargement. These patients can undergo endodontic procedure but over instrumentation should be avoided. Gingival hyperplasia has been reported to be successfully managed with CO2 laser surgery with minimal hemorrhage[29].
It is a challenging task to carry out dental procedures in a SWS patient due to risk of severe intra- and postoperative haemorrhage. Special precautions to keep in mind in order to prevent and treat complications may include hospitalization, application of local anaesthetics with vasoconstrictors, dressings, splints[28]
CONCLUSION
Stupendous scope of clinical manifestations of SWS makes diagnosis a critical task. Patients affected with SWS may or may not exhibit intraoral manifestations. It is crucial for oral health care practitioners’ to have keen and deep rooted knowledge of this rare congenital disorder and exhibit surplus surveillance during routine dental procedures in order to prevent from life’s threatening complication.
Acknowledgement
Special thanks to Dr.Priyanka Vedpathak, Dr. Gaurav Verma, Dr.Manjiri Choudhary, Dr.Apurva Patil, Dr. Akansha Bhandhari, Dr. Kalyani Vaijwade and Dr. Mala Jaisinghani for their valuable contribution.
Disclosure
The authors claim to have no financial interest in any company or any of the products listed in this article.
Conflict of interest :
All authors have none to declare
References:
1. Gorlin RJ, Pindborg JJ.1964. Syndromes of head and neck. New York: McGraw-Hill, pp. 406–9.
2. Welty LD.(2006) Sturge-Weber Syndrome: A Case Study, Neonatal Network:® The Journal of Neonatal Nursing 25(2):89-98
3. Suman Bhagat, Garima Gupta, Sohan Singh.(2015) Unusual presentation of sturge weber syndrome, Journal of case reports 5(1):111-11
4.Ravala Siddeswari, Siddula Manohar, Thatikala Abhilash.(2014) Sturge-Weber syndrome, Journal of Medical & Allied Sciences 4( 2 ): 88-90.
5. Sumit Sen, Sanchaita Bala, Chinmay Halder, Rahul Ahar, Anusree Gangopadhyay. (2015) Pigmentovascularis Presenting with Sturge?Weber Syndrome and Klippel Trenaunay Syndrome, Indian Journal of Dermatology 60(1)
6.Neville BW, Damm DD, Allen CM, Bouquot JE .2009. Oral and Maxillofacial Pathology, 3rd ed, St. Louis: Elsevier.
7. Neto FXP, Junior MAV, Ximenes LS, de Souza Jacob CC, Junior AGR, Palheta ACP.(2008) Clinical Features of Sturge-Weber Syndrome, Intl Arch Otorhinolaryngol 12(4):565-70.
8. Anne-Sophie Dutkiewicz, Khaled Ezzedine, Juliette Mazereeuw-Hautier, Jean-Philippe Lacour, S_Ebastien Barbarot, Pierre Vabres, Juliette Miquel, Xavier Balguerie, Ludovic Martin, Franck Boralevi, Pierre Bessou, Jean-Franc¸ Ois Chateil, And Christine L_Eaut_E-Labr_Eze.(2015) A prospective study of risk for sturge-weber syndrome in children with upper facial port-wine stain, J am Acad Dermatol.
9. Asdullah, Arti S. Sachdev, K.Srinivas, P. Ratnakar.(2015) Sturge-weber syndrome : A case report, University J Dent Scie,1(2)
10. Haslam R.1996 Neurocutaneous syndromes. In: Nelson WE,BehrmanRE, Kliegman RM, Arvin AM, eds. Nelson textbook of pediatrics,15th ed. Philadelphia: W. B. Saunders,1707-9.
11. Natarajan Mannivanan, Subramanium Gokhulathan, Ramakrishna Ahathya, Gubernath, Rajkumar Daniel, Shanmungasundaram.(2012)Sturge –weber syndrome, J Pharm Bioallied Sci 4(Suppl 2): S349–S352.
12. Nathan N, Thaller SR.(2006) Sturge-Weber syndrome and associated congenital vascular disorders: A review, J Craniofac Surg 17:724-8.
13. Comi AM.(2007) Update on Sturge-Weber syndrome: Diagnosis, treatment, quantitative measures, and controversies, Lymphat Res Biol 5:257-64.
14.Bhansali RS, Yeltiwar RK, Agrawal AA.(2008) Periodontal management of gingival enlargement associated with Sturge-Weber syndrome, J Periodontol 79:549-55
15.Chaundhary SC, Sonkar SK, KumarV, Golchha S.(2011)Sturge Weber Syndrome, J Associ Physicians India 59:327-9
16.Khan AN, Turnbull I, Macdonald S, et al. Sturge Weber Syndrome. Available from: http://
emedicine.com
17.The Sturge Weber Foundation: http://www.sturge-weber.org
18. Ankita Pandey, Prasad Yeshwant Deshmukh, Balaji Jadhav, Y. S. Nandanwar.(2015) A rare case of pregnancy with Sturge-Weber syndrome ,Int J Reprod Contracept Obstet Gynecol 4(3):866-868
19. Mustapha adekunle fatai, Adebanjo Oluyemi mary and Aadebimpe Oluwafisayo adenike.(2015) Case Report Sturge-Weber Syndrome: A Case Report in a 39 Yr- Old Man with Delayed Diagnosis , Austin J Clin Neurol 2(6): id1049
20. Paller AS.(1987)The Sturge Weber Syndrome. Pediatric Dermatology 4(4):300-4.
21.Khambete N, Risbud M, Kshar A.(2011) Sturge-Weber Syndrome: A Case Report,International Journal of Dental Clinics 3(1):79-81.
22. Solmaz Abdolrahimzadeh, Vittorio Scavella, Lorenzo Felli, Filippo Cruciani,Maria Teresa Contestabile, and Santi Maria Recupero.(2015) Review Article Ophthalmic Alterations in the Sturge-Weber Syndrome, Klippel-Trenaunay Syndrome, and the Phakomatosis Pigmentovascularis: An Independent Group of Conditions?,Hindawi Publishing Corporation BioMed Research International Volume
23. Wahab Arif, Wahab Shagufta, Khan Rizwan Ahmad, Goyal Ruchi, Dabas Nisha(2008) Sturge Weber Syndrome: A Review Bombay Hospital Journal 50(1):55-58.
24. Godge P, Sharma S, Yadav M, Patil P, Kulkarni S.(2011) Sturge Weber syndrome: A case report, Rev Odonto Cienc 26(4):366-369.
25. Sadick H, Sadick M, Gotte K, Naim R, Riedel F, Bran G, et al.(2006) Hereditary hemorrhagic telangiectasia: an update on clinical manifestations and diagnostic measures ,Wien Klin Wochenschr 118:72–80.
26.Maher ER, Yates JRW, Harries R, et al.(1990) Clinical-Features and Natural-History of von Hippel-Lindau Disease, Quart J Med 77:1151–1163.
27. Elston JB, Payne WG.(2014) Maffucci syndrome. Eplasty 14(ic1):1.
28. D. E. C. Perez, J. S. Pereira Neto, E. Graner, M. A. Lopes.(2005) Sturge–Weber syndrome in a 6-year-old girl, International Journal of Paediatric Dentistry 15:131-135.
29. Darbar UR, Hopper C, Spoight PM.(1982) Combined treatment approach to gingival over growth due to drug therapy, J Clin Periodontol 23: 940
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





