IJCRR - 5(20), October, 2013
Pages: 116-120
Date of Publication: 02-Nov-2013
Print Article
Download XML Download PDF
CHILDHOOD OCULAR EMERGENCIES: 5 YEARS RETROSPECTIVE CLINICAL AUDIT IN A RURAL MEDICAL COLLEGE AND HOSPITAL
Author: Saumen Kumar Chowdhuri, Subhasis Jana
Category: Healthcare
Abstract:Purpose: To evaluate the clinical and epidemiological characteristics of childhood ocular emergency. Materials and Methods: A comprehensive retrospective review was carried out over a period of 5 years from January 2008 to December 2012 at the Dept. of Ophthalmology, Burdwan Medical College and Hospital, West Bengal, India. A total 330 children (aged 15 years or less) was hospitalized with ocular emergencies and included in this study. Results: Total 330 children (aged 15 years or less) were admitted in the inpatient Department of Ophthalmology. Male and female child was 242(73.33%) and 88(26.67%) respectively. Traumatic ocular emergencies was 210(63.64%) where as non-traumatic was 120(36.36%). Male predominance was seen in both group, traumatic 126(60%) and non-traumatic 83(69.2%). Close globe injury 86(40.95%) and open globe injury was 66(31.43%). Hyphema 48(55.81%) was the most common among close globe injury. Corneal rupture 42(63.63%) was most common among open globe injury. Vegetable material was the most common causative agent for traumatic ocular emergency. Non-traumatic ocular emergency was managed with conservative medications and primary repair was done in traumatic open globe injury. Visual outcome was poor in cases of traumatic open globe injury than traumatic close globe injury and non-traumatic group. Conclusion: Childhood ocular emergency is a common cause of ophthalmic consultation. Majority patients are young boys and commonly presented with ocular trauma. There is need for increasing awareness.
Keywords: Audit, childhood emergency, Ophthalmology.
Full Text:
INTRODUCTION
The term audit is “a means of quality control for medical practice by which the profession shall regulate its activities with the intention of improving overall patient care”1. Childhood ocular emergency, commonly ocular trauma is a major cause of acquired monocular visual impairment and blindness in children. Childhood Ocular injuries account for approximately 8-14% of total injury and are the most common type requiring hospitalization2,3. Ocular injury was the 2nd common cause of preventable monocular visual loss in children, next to amblyopia4. Injury was more common in children because of their inability to avoid hazards5. Injury was less frequent in infants and children less than 3 years of age due to close parental supervision6. Accidental injury was more common in older children by toys, pencils, arrows, needles, thorns and stone. Sports related injury was more common in 5-15 years of age7.
MATERIALS AND METHODS
A comprehensive retrospective review was carried out over a period of 5 years from January 2008 to December 2012 at the Department of Ophthalmology, Burdwan Medical College and Hospital, West Bengal, India. All children (aged 15 years or less) admitted with ocular emergency were included in this study. The data was collected from inpatients registers and recorded as traumatic and non-traumatic group. Traumatic ocular injury was further classified as lid injury, closed globe injury, open globe injury, chemical and thermal injury.
Initial visual acuity was measured at the time of presentation. For school-aged children visual acuity was recorded with E chart from 6 meters distance. For preschool children, visual acuity was assessed with the fixation and light follow test pattern.
RESULTS
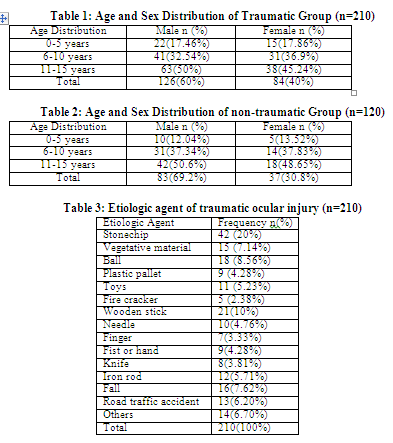
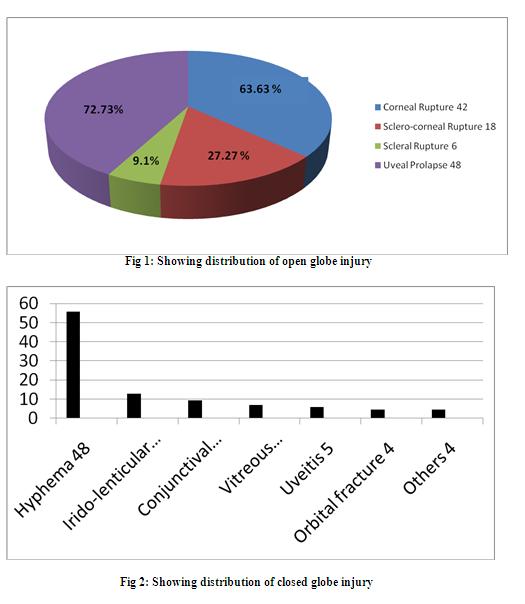
Between January 2008 – December 2012, a total 330 children (aged 15years or less) admitted in the Department of Ophthalmology, Burdwan Medical College and Hospital. Out of these 330 children, 242(73.33%) was male and 88(26.67%) was female. Minimum age of the study patient was 2 month. Traumatic ocular emergencies was 210(63.64%) where as non-traumatic was 120(36.36%). Male predominance was seen in both group, traumatic 126(60%) and non-traumatic 83(69.2%). Table 1 and Table 2 shows the age and sex distribution of traumatic and non-traumatic ocular emergencies respectively. Penetrating trauma was the most frequent mode of injury observed in children. Close globe injury 86(40.95%) and open globe injury was 66(31.43%). Hyphema 48(55.81%) was the most common among close globe injury followed by Irido-lenticular dialysis 11(12.79%). Corneal rupture 42(63.63%) was most common among open globe injury. Fig.1 and Fig.2 shows the distributions of traumatic and non-traumatic childhood ocular emergency respectively. Stone-chip was the most common causative agent for traumatic ocular emergency. Table 3 shows the etiologic agents of traumatic ocular injury. Non-traumatic ocular emergency was managed with conservative medications and primary repair was done in traumatic open globe injury. Visual outcome was poor in cases of traumatic open globe injury than traumatic close globe injury and non-traumatic group.
DISCUSSION
The term audit of surgical outcome could be seen as the final step in what had termed the “journey of care” for the individual patient and for the population as a whole8. Childhood ocular trauma was a leading cause of acquired monocular visual morbidity, accounts for 8-14% of total injury2,3. Because of their immature motor skills and curious nature children are more susceptible to ocular trauma and it was seen that 6-10 years of age was more susceptible9. In the present study we found that male 242(73.33%) was more frequently admitted than female 88(26.67%) Traumatic ocular emergencies was 210(63.64%) more common than non-traumatic 120(36.36%) emergency. Male predominance was seen in both group, traumatic 126(60%) and non-traumatic 83(69.2%). Adhikari et al10 reported that 57% children was male. Penetrating trauma was the most frequent mode of injury observed in this study. Open globe injury 86(40.95%) and close globe injury was 66(31.43%) respectively. Krishnan et al11 reported that 69.20% of traumatic ocular injury was open globe injury and stick (40.31%) was the commonest cause of followed by stone (19.37%). Cornea (89.01%) was the commonest site of perforation followed by sclera (22.54%) and a large proportion of patients had uveal prolapse (78.03%), they also reported that subluxation of lens (38.96%) was commonest than hyphema (27.27%) in blunt injury. Similarly in our study we found that stone 42(20%) was the commonest cause followed by wooden stick 21(10%). Stone was the commonest agent as many stone chips manufacturing industries are located nearby districts and adjacent part of state of Jharkhand. Corneal rupture was seen in 42(63.63%), sclero-corneal rupture was 18(27.27%) and uveal prolapse was seen in 48(72.73%) but in contrast hyphema 48(55.81%) was the commonest finding followed by irido-lenticular dialysis 11(12.79%) in our series. In another study Bukhari et al12 reported that male child (72.25%) was more frequently involved than female child(27.75%). Blunt trauma was most common mode of injury and vegetative material (14.4%) and wooden stick (13.2%). Most common finding was sub-conjunctival hemorrhage (11.5%). Similarly Kaur et al13 reported that penetrating trauma (73.67%) was the most common mode of ocular injury in their study.
Thermal and Chemical injuries, though relatively less frequent are very devastating to the eye. In our study 16 (7.62%) cases were due to thermal or chemical injury.
All cases of lid injury and open globe injury, primary repair was done. Closed globe and thermal/ chemical injuries was managed medically.
Jackson H14 concluded that valid estimation of the annual incidence of infective ulceration was difficult to obtain in most countries. In this study we found that corneal ulcer 56(46.67%) was the most common non-traumatic ocular emergency. Followed by orbit/ adnexal infection 28(23.33%), neuro-ophthalmological 12(10%), endophthalmitis 6(5%), painful red eye 5(4.17%), uveitis 2(1.67%), vitreo-retinal 3(2.5%) causes were in decreasing order of incidence. Majority of the corneal ulcer was due to bacterial 29(51.78%) origin followed by fungus 13(23.21%) and virus 8(14.3%). Gonzales et al15 reported that annual incidence of corneal ulcer in Madurai district, South India was 11.3% per 10,000 populations. Bharathi et al16 found that 32.77% corneal ulcer was due to bacterial agent followed by fungus 34.4% in their study.
In all cases of non-traumatic ocular emergencies, conservative medical management was given.
CONCLUSION
Our study indicates a large number of childhood ocular emergency was admitted in this rural based Medical College and Hospital. Majority was young male who had not received any management before attending the hospital. The prevalence of traumatic ocular injury was higher than non-traumatic group. There is need for increasing awareness among parents, care giver and vulnerable group to reduce ocular morbidity and strict prohibition of child labour in the field of stone chip manufacturing industries.
ACKNOWLEDGEMENT
The authors of this article gratefully acknowledge the inspiration and help received from the scholars whose articles have been cited in the reference section. The authors pay their gratitude to authors/editors/publishers of all those articles/journals/books from where the reviews and literatures for the discussion have been collected.
References:
- Alam SN, Rehman S, Raza SM, Manzar S. Audit of a general surgical unit: Need for self evaluation. Pak J of surgery 2007; 23: 141-4.
- Scribano PV, Nance M, Reilly P, Ronald FS, Steven M. Pediatric Nonpowder Firearm injuries: Outcomes in an Urban Pediatric setting. Pediatrics 1997; 100; e5.
- Takvam JA, Midelfart A. Survey of eye injuries in Norwegian children. Acta Ophthalmol 1993; 71: 500-5.
- Lithander J, Al Kindi H, Tanjum AM. Loss of visual acuity due to eye injuries among 6292 school children in the sultanate of Oman. Acta Ophthalmol 1999; 77: 697-9.
- Negral AD, Thlefors B. The global impact of eye injuries. Ophthalmic epidemiology 1996; 5: 143-69.
- Neranen M, Raivio I. Eye injuries in Children. Br J Ophthalmol 1981; 65: 436-8.
- Mac Ewen CJ, Baines PS, Desai T. Eye injuries in children: The current picture. Br J Ophthalmol 1999; 83:933-6.
- Herbert MA, Prina SL, William SJL. Are unaudited records forming an outcome registry database accurate? Ann Thorac Surg 2004; 77: 1960-4.
- Al-Bdour MD, Azab M. A childhood eye injuries in north Jordan. Int. Ophthalmol 1998; 22: 269-73.
- Adhikari RK, Pokhrel H, Chaudhury H, Chaudhury B.Ocular trauma among children in western Nepal: agents of trauma and visual outcome. Nep J Oph 2010; 2: 164-5.
- Krishnan M, Sreenivasan R. Ocular injuries in union territory of Pondicherry. Clinical presentation. Indian J Ophthalmol 1998; 36: 82-5.
- Kaur A, Agrawal A. Paediatric ocular trauma. Current Science 2005; 89: 43-6.
- Jackson H. Bilateral blindness due to trauma in Combodia. Eye 1996; 10: 517-20.
- Bharathi MJ, Ramakrishnan R, Vasu S, Meenakshi R, Shivkumar C, Palaniappan R. Epidemiology of bacterial keratitis in a referral centre in south India. Indian Journal of Medical Microbiology 2003; 21: 239-45.
- Bukhari S, Mahar PS, Qidwai U, Bhutto IA, Memon AS. Ocular Trauma in Children. Pak J Ophthalmol 2011; 27: 208-13.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





