IJCRR - 5(20), October, 2013
Pages: 105-108
Date of Publication: 02-Nov-2013
Print Article
Download XML Download PDF
VARIATIONS IN THE BRANCHING PATTERN OF CAROTID ARTERIAL SYSTEM: CASE REPORT
Author: Sharmadha K.L. Sujana M., Arvind yadav, Pushpalatha M., Meenakshi Parthasarathi
Category: Healthcare
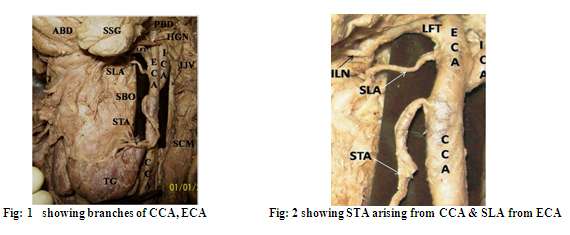
Abstract:The external carotid arterial system is a complex vascular system constituting the nourishment to territorial areas of the head, face and neck tissues. Though the variation in the carotid arteries and their branches are common in the carotid triangle, it is important for the clinicians, surgeons and the radiologists to be aware of all possible variations of these arteries. This paper is an endeavor to bring to notice a rare variation which has immense radiological and surgical importance. In present case \? Left superior laryngeal artery (SLA) was arising from External Carotid Artery (ECA) instead of Superior Thyroid Artery (STA) in the cadaver of an approximately 70 year old Asian male. In addition STA arose from Common Carotid Artery (CCA) 2cm before bifurcation instead of ECA. From ECA the lingual and facial arteries arose from common facio-lingual trunk.
Keywords: STA, SLA, ECA, CCA, Hemodynamics, facio-lingual trunk.
Full Text:
INTRODUCTION
It is important for surgeons and radiologist to be aware of the normal anatomy of CCA, ECA and their branches. Variations among these vessels are quite common, it became further essential to know and report all the probable variations [1].
The detail knowledge of the gross and radiologic anatomy of ECA with its branches is essential for application of angiography in the diagnosis of lesion affecting the neck, face, scalp and dura. The abnormalities most readily diagnosed are tumors, vascular malformations or bony disorders [2].
Understanding the surgical anatomy of STA is necessary for successful radical neck dissection and to minimize postoperative complications in the bloodless surgical field such as emergency cricothyroidotomy, radical neck dissection, catheterization, reconstruction of aneurysms and carotid endarterectomy [3].
CASE REPORT
During routine dissection for medical undergraduate teaching in the department of Anatomy, faculty of medicine, BMCRI, Bangalore. We found 3 variations in the arteries of left aortic arch of an approximately 70 year old Asian man.
The CCA was divided into ECA & ICA at the level of lamina of the thyroid cartilage. STA was arising from CCA about 2cm proximal to the bifurcation, SLA was arising from ECA 6mm distal to the bifurcation of CCA. The lingual and facial arteries originated from ECA as a facio-lingual trunk. The remaining branches of ECA were normal in origin. The arterial system was dissected carefully and photographed. Other structures of carotid triangle were normal. The CCA was 10cm long.
DISCUSSION
It is universally accepted that CCA divided into ECA & ICA at the level of superior border of thyroid cartilage.
Ilic found this to be true in 58% of cases, in 25% carotid bifurcation is at the level of inferior border of hyoid bone. A higher bifurcation opposite to superior border of hyoid bone was found in 12.5%, bifurcation appeared at the level of inferior of the thyroid cartilage in 12.5% [5].
In this cadaver the CCA bifurcation was found to be almost at the level of lamina of superior border of throid cartilage.
The STA is frequently used as a recipient vessel for microvascular free tissue transfer in head and neck surgery, for selective embolization of thyroid and head and neck tumors, and as a landmark for identifying the external branch of SLA in thyroid surgery [6].
Lo et al. reported that the origin of STA appeared to be related to the level of the CCA bifurcation [7]. When CCA had a relatively low bifurcation, such as at the lamina of the thyroid cartilage, the STA tended to originate from the ECA. In contrast, when the CCA had a high bifurcation, the STA tended to originate from the CCA. In the present case CCA was 10cm long. But, the mean length of the left CCA has been reported to be 12.1 ± 0.2 cm [8]. This suggests that the CCA in our case was short, which means there was a low bifurcation. This finding is not consistent with the observations of Lo et al. [7].
In rare cases, the SLA might arise from the lingual, facial or ascending pharyngeal arteries [9]. The distance of origin of the SLA from the carotid bifurcation in cases in which the artery arises from ECA has been reported by Vazquez et al. [6]. In their study they have reported 4 different origins for the SLA, the most frequent type being from the carotid bifurcation (49%). Similarly, they have reported 4 different origins for the SLA and most frequent type is one in which the artery arose from STA (78%). Lucev et al. reported that STA arise more often from CCA (47.5%) than from ECA (30%) [5].
In this case first branch of ECA is SLA, so this variation must be kept in mind. The accepted site of ECA ligation is inferior to the origin of STA. However its closeness with CCA bifurcation might cause difficulty in surgery and it is accepted that ligation above STA may preserve good collateral circulation [6].
Developmental aspect
The development of the ECA system is a complicated process of angiogenesis and remodeling which includes annexation and regression of vessels. The development of hypostapedial artery which links the neural crest arterial system to the ventral pharyngeal artery marks an important event in the development of ECA system [10].
- The dorsal remnant of the second aortic arch forms hyoid artery, at 9mm stage of the embryo. It arises from the dorsal aorta which later forms the petrous segment of ICA.
- At 16mm stage of the embryo, the hyoid artery gives of an ascending branch called stapedial artery.
- At this stage the various ventral vestigies of the first and second aortic arch arteries and ventral aorta form ventral pharyngeal artery which later forms the stem of external carotid system [10].
Varients will result from deviations in this program. The signals involved in annexations and regressions are not always synchronized and as a result the vascularization varies.
Hemodynamic aspect
The hemodynamic balances in the maxillofacial and submandibular regions which are nourished by the anterior extracranial carotid branches require to be analyzed [2].
Linguofacial collateral pattern
Three principal arterial trunks are distributed to these regions: facial artery, lingual artery and superior thyroid artery [2]. These arteries form an arterial circle arpund the sublingual gland. In case, simultaneously if both the facial and lingual arteries or a common faciolingual trunk is not congenitally developed and unable to nourish there territory the blood supply will be recruited by ipsilateral collateral pathways from superior thyroid branches.
Clinical importance And Conclusions
Profound knowledge of the anatomical characteristics and variations of the carotid artery, such as its branching pattern and position is essential to avoid complications which catheter insertion of carotid arteries in various procedures. Variations in patterns of origin, courses and branching pattern of the STA during surgical procedures in the neck region, such as during emergency cricothyroidotomy, radical neck dissection, carotid catheterization, reconstruction of aneurysm and carotid endarterectomy.
Abnormalities observed in our case, adds to the long list of known variations of these arteries and could help avoid serious implications during radiological examinations, interventions, ultrasound examination, exploration of the neck, thyroid and parathyroid surgery, tracheotomy, surgery of the larynx, pharynx and upper esophagus and microvascular surgeries [5].
References:
- Mohan Rao KG,Vincent Rodrigues, Koshy Shajan. Unilateral high origin of facial artery associated with a variant origin of the glandular branch to the submandibular gland.IJAV.(2008) 2; 136-137.
- Madhuri Avinash Mahendrakar. Variation in the branching pattern of external carotid artery: a case report. J.anat.soc.india2007, 56(2); 47-51.
- BV. Murulimanju,et al. Variations in carotid arterial system. Chang gung Med j.(2012) 35(3);281-284.
- Rao Mohandas KG, Rao Asutosh S. Unusual origin of the arteries in the carotid triangle of neck. The open Anatomy journal.2009,1,24-27.
- Lucev N, Bobinac D, Maric I, Variations of the great arteriesin the carotid triangle. Otolaryngol Head Neck 2000;122:590-1.
- Vazquez T, Cobiella R, Maranillo E.Anatomical variations of the superior thyroid and superior laryngeal arteries. Head neck 2009;31:1078-85.
- Lo A, Oehley M, Bartlett A. Anatomical variations of the common carotid artery bifurcation. ANZ J Surg 2006;76:970-2.
- Ribeiro RA, Ribeiro JAS, Rodrigues Filho OA. Caetanoels related to clinical relevant anatomical landmarks. Int J Morphol 2006;24:413-6.
- Nayak SB, Soumya KV. Neurovascular variations in the carotid triangle. IJAV 2008;1:17-8.
- Larsen WJ: Human embroyology. 2nd Edn; Churchill Livingstone New York, Edinburgh, London,1997.191-195.
- Mohan Rao KG,Vincent Rodrigues, Koshy Shajan. Unilateral high origin of facial artery associated with a variant origin of the glandular branch to the submandibular gland. IJAV. (2008) 2; 136-137.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





