IJCRR - 5(22), November, 2013
Pages: 94-99
Date of Publication: 04-Dec-2013
Print Article
Download XML Download PDF
IMPORTANCE OF TUBERCULOSIS IN GLOBAL HEALTH AGENDA-AN EPIDEMIOLOGICAL STUDY OF TUBERCULOSIS AMONG MIGRANT POPULATION FROM SOUTH EAST ASIA, MIDDLE EAST and AFRICAN REGIONS TREATED WITH WHO-DOTS REGIMEN
Author: Vijay Kumar Chattu, Mohammad A.
Category: Healthcare
Abstract:Objective: To study the epidemiology and clinical characteristics of Tuberculosis among Saudis and migrant population in Saudi Arabia. Methods: Retrospective study was conducted based on the secondary data pertaining to the patients registered at Regional TB center in Buraidah Central Hospital from January 2005 to December 2009. Results: A total of 355 case records were included of which 187 cases are from Saudi Arabia and remaining 168 were from South Asian, African and Middle East countries. All the diagnosed cases were treated as per WHO- DOTS regimen. Cough with expectoration, fever with evening rise, loss of appetite were the chief clinical presentations. Out of the total non Saudi patients, the Indonesian patients contribute to 74 (21%) followed by Indians 39 (11%), Nepalese 12 (3.4%), Philippines and Bangladesh with 9 cases each (2.5%), and Pakistan with 8 cases (2.3%). Among the total cases, there were 341 (96%) new cases, 12 (3.4%) relapse cases and 2 (0.6%) defaulters. Conclusion: Prevalence of TB among migrant is relatively high. Preventive measures for early diagnosis should be performed especially in migrant worker from high-prevalence countries.
Keywords: Prevalence, Tuberculosis, Retrospective Study, South Asia
Full Text:
INTRODUCTION
Global health is the health of populations in a global context and transcends the perspectives and concerns of individual nations. In global health, problems that transcend national borders or have a global political and economic impact are often emphasized. Thus, global health is about worldwide improvement of health, reduction of disparities, and protection against global threats that disregard national borders. Tuberculosis (TB) has troubled humankind throughout history. Tuberculosis (TB) is an ancient disease that has affected mankind for more than 4,000 years. It is a chronic disease caused by the bacillus Mycobacterium tuberculosis and spreads from person to person through air. TB usually affects the lungs but it can also affect other parts of the body, such as brain, intestines, kidneys, or the spine. Although a declining trend was observed in most developed countries, this was not evident in many developing countries. Global health is now considered important for national and international security, domestic and global economic well-being. In 2011, there were an estimated 8.7 (range, 8.3–9.0 million) million incident cases (equivalent to 125 cases per 100 000 population) of TB globally [1]. M. tuberculosis is known to be the leading cause of death due to a single infectious agents [2, 3 and 4]. The worldwide annual incidence continues to increase in Africa with 85% new cases because of the human immune deficiency virus HIV epidemic, whereas it is stable or falling in all other regions [5]. Although the majority of infected individuals don’t exhibit overt signs of disease, they represent a large pool of infection that allows for new cases to arise and have a risk of reactivation at a later time in their lives [6]. The risk increases significantly when the immune system of infected individual becomes suppressed, such as individuals infected with HIV [7, 8].
An accurate description of TB is difficult to obtain because of poor diagnostic facilities and reporting systems in many countries where infection is dominant [9]. The best information available on global TB comes from the World Health Organization (WHO) with Southeast Asia holding the highest number of people infected with TB in the world (World Health Organization, 2003).
Cases of pulmonary TB constituted 70.6% while the extra-pulmonary TB cases constituted 29.4% of the total cases in this year [10]. In addition, Saudi Arabia in general with its developmental projects is known to attract a lot of international work force from Asian and African countries where infections might be dominant. Therefore, this study was carried out aiming to determine epidemiological and clinical characteristics of TB cases among general population in Qassim region, Saudi Arabia between January 2005 and December 2009 and to provide valuable insight on pulmonary and extra- pulmonary TB.
MATERIALS AND METHODS
Study population and Data collection
This study was conducted in a regional TB center in Qassim region that lies approximately at the centre of the Arabian Peninsula. It was conducted as a retrospective study based on the secondary data pertaining to the patients registered in hospital from January 2005 to December 2009. Out of 400 cases, the records were scrutinized and completeness of the data available for 355 cases were included and analyzed for the present study. A total of 355 patients registered at the hospital were included in the study. The patients registered at this hospital were coming from all the parts of Al Qassim province which is a representative sample. Patients' case sheets were used as source of data. A detailed questionnaire including the information on socio economic conditions (like income, close contacts, living conditions), personal history (including smoking, alcohol, drug abuse, HIV infection etc) and clinical history was developed and these variables were analyzed in the study to give a clear picture of epidemiology of TB in the region. Findings were cross-checked with TB-Lab register, TB register, and TB cards of patients. Apart from demographic profile of the patients, the presenting symptoms, co-morbid conditions, diagnostic methods used and treatment regimen were also assessed. The cases were diagnosed by the medical officer of the hospital as per the WHO classification using the direct sputum examination and chest X-ray. Montoux test was also done on all the patients.
Ethical consideration and Statistical analysis
The study was approved by the Ethics and Research Committee of Qassim University and the hospital authorities of TB regional center. Data collected through structured questionnaires is entered and analyzed using Epi_info software (CDC Atlanta). Simple proportions and percentage were used as statistical methods.
RESULTS
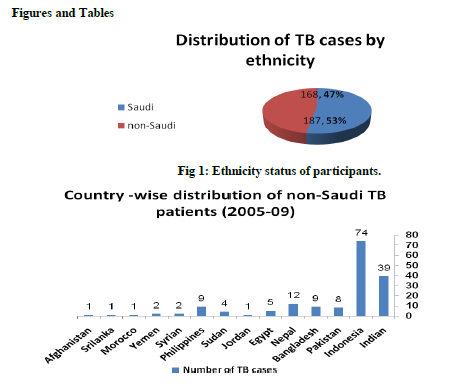
A total of 355 patients with TB and other co-morbid conditions accessing the TB services at regional TB center at Qassim comprised the study population. Of the 355 patients, Saudi ethnicity observed in 187 (52.7%) patients compared to non Saudi 168 (47.3%) as shown in figure 1. Out of the total non Saudi patients, the Indonesian patients contribute to 74 (21%) followed by Indians 39 (11%), Nepalese 12 (3.4%), Philippines and Bangladesh with 9 cases each (2.5%), and Pakistan 8 (2.3%). There were few patients from other countries like Sudan, Egypt, Jordan,
Srilanka, Syria, Afghanistan and Morocco as shown in figure 2.
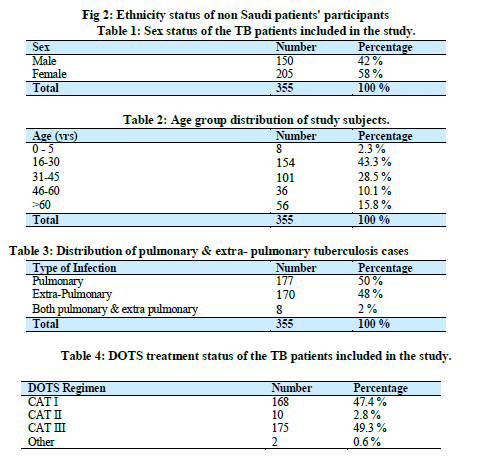
Among the total number of patients diagnosed with TB, 150 (42 %) were males and 205 (58 %) were females (Table 1) with the majority of participants 154 (44%) being in the age group of 16-30 years and 101 (28.5%) being in the age group of 31 – 45 years as shown in Table No. 2.
Nearly half of these cases 177 (49.9%) are pulmonary TB, and the other half were divided between 170 (47.9%) were extra-pulmonary cases and 8 (2.2%) cases with both pulmonary and extra-pulmonary involvement as shown in Table 3.
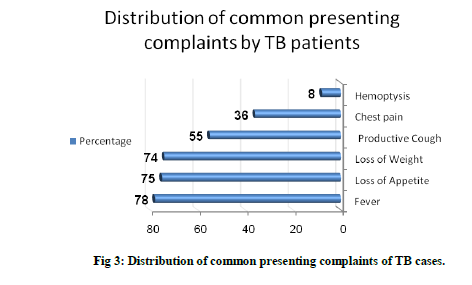
Patients included in this study with both pulmonary and extra pulmonary TB had various clinical presentations but they had complaints similar to the typical TB case presentation. The majority of patients 278 (78.3%) were admitted with fever, 266 (74.9%) had loss of appetite, 264 (74.4%) had loss of weight, 196 (55.2%) complaining of cough with expectoration and 128 (36.2%) were presenting with chest pain as shown in Figure 5. In addition there were co-morbid conditions associated like Diabetes mellitus in 36 cases (10%), and 12 (3.5%) patients were suffering from lung disease and 6 (1.7%) suffering from chronic renal failure as shown in figure 3.
All the cases were treated with Directly Observed Treatment Short course (DOTS) regimen of WHO. Out of total 355 patients on DOTS, 168 (47.3%) patients were put under CAT I, 10 (2.8%) CAT II and 175 cases (49.3%) CAT III. There were 341 (96%) new cases and 12 (3.4%) relapse cases and 2 (0.6%) defaulters among the total patients (table 4).
DISCUSSION
Over the last few decades, considerable effort has been expended in industrialized countries to control the spread of TB. A lot of these processes were effective initially [11]. In the USA, for instance, the incidence of TB decreased by 6% yearly [12]. However, TB remains to be a major health concern throughout the world. It is critical for TB control and surveillance programs to address the burden of TB in certain population. Previous reports have indicated that the incidence of smear-positive TB in Saudi Arabia was estimated to be 20 per 100,000 populations [13]. Neighboring countries such as United Arab Emirates have similar rate of TB incidence.
Our study provides population-based data on the TB cases in Qassim region, Saudi Arabia from 2005 to 2009. As shown approximately, 47.3% of TB cases included in this study are attributed for non Saudi patients indicating the important role that migrants play in TB epidemiology in Saudi Arabia [14]. Majority of migrants were from TB-high burden countries, which is one of the important factors that contribute to resurgence of the disease. Therefore, screening migrants form countries endemic for TB is valuable to significantly reduce the spread of infection according the national guidelines [15]. The high prevalence of extra-pulmonary TB in the study in comparison to overall of Saudi Arabia of 29.4% is probably due to the high number of females immigrating to Saudi Arabia as housemaids from the TB-high burden countries. Nearly half of these cases 177 (49.9%) are pulmonary TB, and the other half were divided between 170 (47.9%) were extra-pulmonary cases. There were other co morbid conditions like Diabetes mellitus in 36 cases (10%), 12 (3.5%) patients were suffering from lung disease and 6 (1.7%) suffering from chronic renal failure
Our data suggested that approximately 73% of subjects participated in this study belong to the age group of 16 – 45 years old proving that TB is a disease of economically productive age group among the low socio-economic strata of the society which goes in agreement with previously published study [16]. TB symptoms and clinical presentation of the present study were typical of TB cases with the majority of patients complained of Fever, loss of appetite, loss of weight, and cough with expectoration.
The positive aspect of this study was that doctors working at the Regional Hospital were following the WHO-DOTS regimen for the diagnosis and treatment of even complicated cases of TB.
CONCLUSION
In conclusion, in the current study, we examined the incidence and the pattern of TB cases registered in Qassim TB center and the findings of this study revealed the high prevalence of TB among migrants mainly those from Southeast Asia. Further studies and continued surveillance of the TB infections are required to formulate plans for the effective management of TB.
ACKNOWLEDGMENT
Authors would like to thank the members of Tuberculosis Regional Center at Buraidah Central Hospital who gave their full cooperation and support for this study. Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
Conflict of interest: The Authors declare that there is no conflict of interest
Source of Funding: This research work is supported by a grant from the Scientific Research Deanship at Qassim University, Saudi Arabia 2009.
Ethical clearance: The study got ethical clearance from the Ethics and Research Committee of Qassim University
References:
- The seventeenth global report on tuberculosis, Global Tuberculosis report 2012 http://www.who.int/tb/publications/global_report/gtbr12_annex4.pdf (accessed in June 2013)
- Murray, C. and Feachem, R. (1990) Adult mortality in the developing world. Trans R Soc Trop Med Hyg 84(1):21-22.
- Styblo, K. (1980) Recent advances in epidemiological research in tuberculosis. Adv Tuberc Res 20:1-63.
- Murray, C., DeJonghe, E., Chum, H., Nyangulu, D., Salomao, A., and Styblo, K.(1991) Cost effectiveness of chemotherapy for pulmonary tuberculosis in three sub-Saharan African countires. Lancet; 338(8778):1305-1308.
- WHO. Global tuberculosis control: surveillance, planningand financing. Geneva, 2006: WHO/HTM/TB/2006.362.
- Chamie, G., Luetkemeyer, A., Charlebois, E. and Havlir, D. (2010) Tuberculosis as Part of the Natural History of HIV Infection in Developing Countries. Clin Infect Dis. 15;50 Suppl 3:S245-54.
- Harries, A. and Dye, C. (2006) Tuberculosis. Ann. Trop. Med. Parasitol. (100): 415-431.
- Dye, C. (2006) Global epidemiology of tuberculosis. Lancet. (367): 934-940.
- Bentrup, K. and Russell, D. (2001) Mycobacterial persistence: adaptation to a changing environment. Trends in Microbiol. (9): 597-605.
- Khaled NA, Enarson D, Bousquet J. Chronic respiratory diseases in developing countries: The burden and strategies for prevention and management. Bulletin of the World Health Organization. Print ISSN 0042-9686. Geneva; 2001.
- Health Statistics Book Year 2006 Ch -1 review of health situation, III: Chest Diseases.
- Raviglione MC, Snider Jr. DE, Kochi A. Global epidemiology of tuberculosis. Morbidity and mortality of a worldwide epidemic. JAMA 1995; 273:220–6.
- Snider Jr. DE, Roper WL. The new tuberculosis. N Engl J Med 1992; 326:703–5.
- Global tuberculosis control: WHO reports 1996-2002. Available at: www.emro.who.int/stb/TBSituation-CountryProfilesaa.htm. [Accessed Aug 1, 2009]
- Zaman R. Tuberculosis in Saudi Arabia: epidemiology and incidence of mycobacterium tuberculosis and other mycobacterial species. Tubercle 1991; 72: 43-9.
- Tulsky JP, White MC, Dawson C, Hoynes TM, Goldenson J, Schecter G. Screening for tuberculosis in jail and clinic follow-up for after release. Am J Public Health 1998; 88: 223-6.
- Bahl R, Singh B, Singh R: Prevalence of HIV infection among patients of pulmonary tuberculosis attending chest disease hospital, Jammu and Kashmir; Ind J of Community Med, 2007; 32 (4): 288-289
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





