IJCRR - 5(22), November, 2013
Pages: 46-50
Date of Publication: 04-Dec-2013
Print Article
Download XML Download PDF
SUPRASCAPULAR NOTCH VARIATIONS AND ITS CLINICAL SIGNIFICANCE
Author: Aradhyula Himabindu, B. NarasingaRao, Nihar Sannala
Category: Healthcare
Abstract:Aim: The suprascapular nerve that lies in the suprascapular notch of scapula requires special attention as it supplies muscles which initiate abduction of the shoulder. From its origin in the upper trunk of the brachial plexus, the suprascapular nerve passes through the suprascapular notch to supply the supraspinatus later it passes through the spinoglenoid notch to supply the infraspinatus. During its course there is a chance of entrapment of the nerve in the suprascapular notch due to its different shapes and dimensions which leads to suprascapular nerve entrapment syndrome. Materials & Methods: The present study was done on 43 dried human scapulae. The suprascapular notch was observed in each bone to find out variations in its shape. Results: This study showed three different types of suprascapular notches. The scapulae showed U, V, & J shaped notches, foramen formed by ossification of the transverse scapular ligament, and coexistence of notch and foramen due to ossification of the anterior coracoscapular ligament. Conclusion: These variations in the suprascapular notches are a great help to clinicians for early diagnosis of suprascapular nerve compression.
Keywords: scapula, suprascapular nerve, suprascapular notch, transverse scapular ligament
Full Text:
INTRODUCTION
The scapula is a flat bone of shoulder girdle that lies on the posterolateral aspect of the thorax. In the superior border of scapula, there is a suprascapular notch which is bridged by transverse scapular ligament converting into foramen. The suprascapular nerve passes through this foramen and supplies the supraspinatus and infraspinatus which initiate abduction movement. The variations in the shape and dimensions of the suprascapular notch associated with partial or complete ossification of the superior transverse scapular ligament lead to compression of nerve in the notch against the suprascapular ligment during abduction leading to suprascapular nerve entrapment syndrome. Koepell and Thomson were the first to describe the suprascapular nerve entrapment syndrome.(1) Many authors proposed different classifications . Based on the shape Ticker and collegues (2) defined two types of suprascapular notches-U&V and Iqbal (3) defined three types-U, V&J.
A new classification based on parameters such as vertical and transverse diameters of suprascapular notch was proposed by Natsis et al (4). The present study is done on the basis of classification proposed by Iqbal and Natsis et al. These variations will help the clinicians to determine the type of notch and the possibility of suprascapular nerve entrapment.
MATERIALS AND METHODS
The study is conducted on 43 dried scapula of both sides from the department of anatomy, Maharaja’s Institute of Medical Sciences, Nellimarla, Vizianagarum. Variations in the shapes of suprascapular notch were noted. The vertical and transverse dimensions were measured to classify the notch according to Natsis et al. Transverse diameter is the distance between the two edges of the notch and vertical diameter is the distance between the deepest point of the notch to the midpoint of the line joining the two edges of suprascapular notch.
OBSERVATIONS
The present study followed the classifications of Iqbal (3) and Natsis et al (4) to read the suprascapular notch in detail. In this study three different types of notches are observed along with partial or complete ossification of transverse scapular ligament.
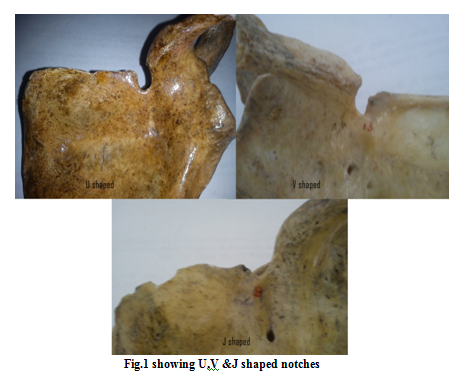
The scapulae are grouped depending on the shape of the notch following the Iqbal classification. Of these scapulae, 29 showed U shaped, 5 J shaped and 3 V shaped suprascapular notches (Fig.1)
But in this classification the author did not mention ossification of the transverse scapular ligament, where two bones with U shaped notches showed partial ossification on the medial side of the notch, five bones showed complete ossification and one bone showed a rare feature of coexistence of notch and foramen. In this last bone, an ossified band is seen extending from root of coracoid process to the middle of suprascapular notch forming a foramen below the band and notch above the band.
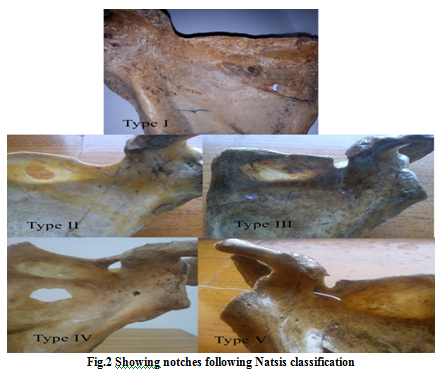
The present study also followed the Natsis et al classification that was based on the dimensions of the suprascapular notch. This study observed 3 scapulae without a discrete notch (Type I), 26 scapulae showed notches where transverse diameter is more than vertical (Type II), in 8 scapulae vertical diameter is more than transverse diameter (Type III), 5 scapulae had ossification of transverse scapular ligament converting the notch into foramen (Type IV) and only one scapula presented with coexistence of notch and foramen(Type V). (Fig.2)
DISCUSSION
Many authors classified SSN based on certain parameters.
Based on gross examination of its shape, Ticker and collegues (2) described only two types of notches- U& V and Iqbal (3) defined three types-U, V & J.
Depending on the inferior shape of suprascapular notch and the degree of ossification, Rengachary et al(5) classified SSN into six types.
Type I- Wide depression in the superior border of the scapula
Type II- Wide blunted V shape, Type III- Symmetric U shape
Type IV-Very small V shape, often with a shallow groove for the suprascapular nerve
Type V- Partial ossified medial portion of the suprascapular ligament
Type VI- Completely ossified suprascapular ligament
The present study not followed this classification as there is no description of coexistence of notch and foramen.
Natsis et al (4) proposed a simple classification based on the vertical and transverse dimensions of the notch.
Type I- without a discrete notch,
Type II- a notch that was longest in its transverse diameter,
Type III- a notch that was longest in its vertical diameter,
Type IV- a bony foramen
Type V- a notch and a bony foramen
The size of the suprascapular notch plays a role in the impingement of the nerve in the notch. A small notch has higher chances of suprascapular nerve entrapment than a large notch (5). In various cases it was identified that partial or complete ossification of the transverse scapular ligament is the predisposing factor for suprascapular nerve entrapment (2, 6, 7). As the ossified ligament decreases the size of the notch and reduces the space available to the nerve, there is a higher chance of suprascapular nerve entrapment (8). The rare occurrence of the coexistence of suprascapular notch and foramen was first reported by Hrdicka (9) in 1942. Later Natsis et al.(4) reported this feature in his study on 423 dried scapulae. Sinkeet et al.(8) described one case suprascapular notch and foramen in his study on Kenyan population.
The present study predominantly showed Natsis type II suprascapular notches where the transverse diameter is more than the vertical diameter and Iqbal U- shaped notches. In this type of notch there was less chance of suprascapular nerve entrapment syndrome as more space is available for the suprascapular nerve. Along with this the present study also showed a scapula with an ossified transverse suprascapular ligament and that a bone with a rare feature of coexistence of notch &foramen (anomalies). These cases are more prone to suprascapular nerve entrapment due to narrowing of the space for the suprascapular nerve which irritates the nerve during different shoulder movements. (5)
Avery et al (10) first described an additional fibrous band anterior coracoscapular ligament in American population. It is arranged either parallel or obliquely to superior transverse scapular ligament in the suprascapular notch. Later Bayramogluet al(11) found this in Turkish population and recently Piyawinijwong et al (12)in Thai population.
Based on anatomical findings of Avery et al (10), Michal Polgrej.et al.(13) explained the cause for the coexistence of notch and foramen. If ossification occurs only in anterior coracoscapular ligament without affecting superior transverse scapular ligament, it leads to coexistence of notch and foramen reducing the space for the nerve. So the nerve is irritated by the bony margins and increases the risk of suprascapular neuropathy.
CONCLUSION
The suprascapular nerve is closely related to the superior border of the scapula as it passes through the suprascapular notch to innervate muscles. Due to variations in the shape of the notch and ossification of the suprascapular ligament the space available to the nerve decreases leading to suprascapular nerve entrapment syndrome. This causes pain over the shoulder as the nerve supplies the supraspinatus and infraspinatus which initiates abduction of shoulder joint. The present study described different types of suprascapular notches. Of these, U shaped notches have lower chances and ossified transverse scapular ligament have higher chances of impingement of the suprascapular nerve. These anatomical variations can be defined by plain radiographs, so that, the clinicians can easily correlate the nerve entrapment with the type of notch.
References:
- Kopell HP, Thompson WA. Pain and the frozen shoulder. Surg Gynecol Obstet 1959;109: 92-96.
- Ticker JB, Djurasovic M, Strauch RJ, April EW, Pollock RG, Flatow EL et al. The incidence of ganglion cysts and variations in anatomy along the course of the suprascapular nerve. J. Shoulder Elbow Surg. 1998; 7(5):472-8.
- Iqbal K, Iqbal R, Khan SG. Anatomical variations in shape of suprascapular notch of scapula. J. Morphol. Sci. 2010; 27:1-2.
- Natsis K, Totlis T, Tsikaras P, Appell HJ, Skandalakis K. Proposal for classification of the suprascapular notch: a study on 423 dried scapulas. Clin. Anat. 2007; 20:135-139.
- Rengachary SS, Burr D, Lucas S, Khatab HM, Mohn MP, Matzke H. Suprascapular entrapment. neuropathy: a clinical,anatomical and comparative study, Part 2: anatomical study. Neurosurg. 1979; 5:447-451
- Alon M, Weiss S, Fishel B, Dekel S. Bilateral suprascapular nerve entrapment syndrome due to an anomalous transverse scapular ligament. Clin Orthop 1998; 234:31-33.
- Cohen SB, Dines DM, Moorman CT. Familial calcification of the superior transverse scapular ligament causing neuropathy. Clin Orthop 1997; 334:131-135.
- S.R. Sinkeet, K.O. Awori, P.O. Odula, J.A. Ogeng’o, P.M. Mwachaka The suprascapular notch: its morphologyand distance from the glenoid cavityin a Kenyan population Folia Morphol.Vol. 69, No. 4, pp. 241–245
- Hrdicka A (1942) The adult scapula: additional observations and measurements. Am J Phys Antropol 29:363–415
- Avery BW,Pilon FM,Barclay JK Anterior coracoscapular ligament and suprascapular nerve entrapment.Clin Anat 2002,15:383-386
- Bayramog?lu A, Demiryu¨rek D, Tu¨ccar E, Erbil M, Aldur MM, TetikO, Doral MN (2003) Variations in anatomy at the suprascapularnotch possibly causing suprascapular nerve entrapment: ananatomical study. Knee Surg Sports Traumatol Arthrosc11:393–398
- Piyawinijwong S, Tantipoon P (2012) The anterior coracoscapularligament in Thais: possible etiological factor of suprascapularnerve entrapment. Siriraj Med J 64:S12–S14
- Michal Polguj.Kazimierz Jedrzejewski.Agata Majos.Miroslaw Topol Coexistance of the suprascapular notch and the suprascapular foramen-a rare anatomical variation and a new hypothesis on its formation based on anatomical and radiological studies Anat Sci Int 2013 88:156-162.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





