IJCRR - 5(23), December, 2013
Pages: 49-52
Date of Publication: 16-Dec-2013
Print Article
Download XML Download PDF
VULVAR CANCER WITH BONE METASTASES: A RARE CASE REPORT
Author: Saptarshi Ghosh1, Sivasankar Kotne, Samir Ranjan Nayak, SPV Turlapati
Category: Healthcare
Abstract:Purpose - Vulvar carcinoma with bone metastases is an extremely rare entity with only twelve cases reported in literature till date. We report a case of squamous cell carcinoma vulva with multiple bone metastases. Case - A 32 year old female presented with a Stage IIIB (FIGO Classification) vulvar malignancy, in which radical vulvectomy with bilateral Ilio-inguinal lymphadenectomy was done. Four weeks later the patient presented with pain in the left shoulder region which was proved to be metastases later. She was started on palliative radiation therapy and palliative chemotherapy. Conclusion \? History of bone pains in patients with gynaecological malignancies should always be investigated properly so as not to miss such uniquely aggressive presentation, especially in higher stage diseases. Here, a patient with well differentiated squamous cell carcinoma vulva developed multiple osseous metastases within a month following surgery.
Keywords: Squamous cell carcinoma vulva; Multiple bone metastases; Radical vulvectomy; Bilateral Ilio-inguinal lymphadenectomy.
Full Text:
INTRODUCTION
Vulvar cancer accounts for about 4% of all gynaecological malignancies. Like other gynaecological malignancies, vulvar cancer spread mainly through the lymphatic rather than the hematogenous route. [1] Vulvar cancer with hematogenous bone metastases is an extremely rare presentation with only twelve cases reported in literature till date, of which all women were of age greater than 50 years. Bone metastases in gynaecological malignancies are often under-diagnosed. [2] The presence of bone metastases in vulvar carcinoma alters the management protocol of the treating oncologist, thereby warranting the need for palliative radiotherapy and palliative chemotherapy. It also marks a very poor prognostic signature for the patient. So it is gravely important to take a plain radiograph of the affected site when a patient with gynaecological cancer complaints of bone pain and rule out the rare possibility of bone metastases in such cancers.
CASE REPORT
We report a 32 year old female who presented with complaints of burning sensation and itching in the clitoris of six months duration. Clinical examination revealed a 2.5cm x 2.0cm ulcerative lesion at the clitoris and bilateral inguinal lymphadenopathy. Histopathological examination
revealed a well differentiated squamous cell carcinoma of the vulva.
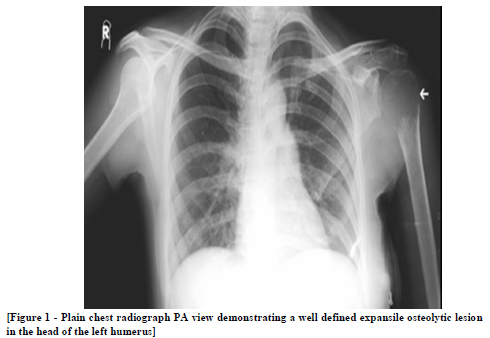
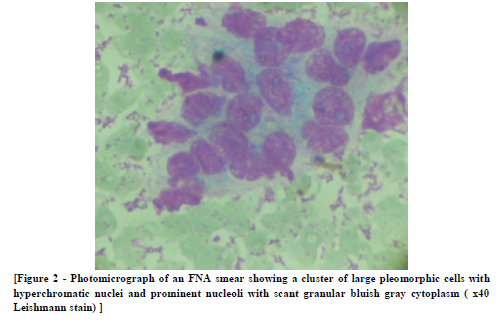
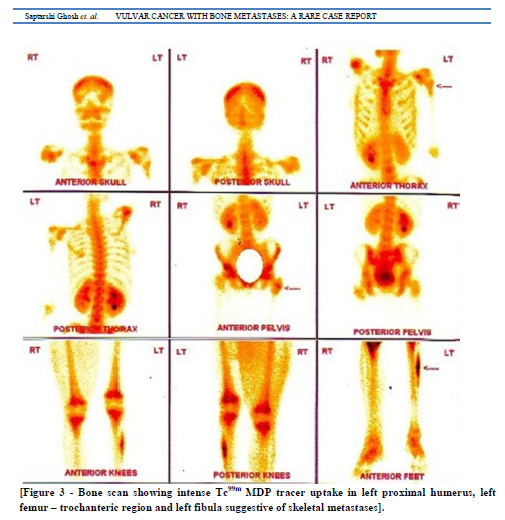
The patient underwent radical vulvectomy and bilateral Ilio-inguinal lymphadenectomy. Postoperative histopathology confirmed metastatic squamous cell carcinomatous deposits in bilateral inguinal lymph nodes - pT1b, pN2a, M0; G1(FIGO Stage III B) vulvar carcinoma. She was advised for adjuvant radiation six weeks post-surgery, following wound healing. But the patient presented earlier, only four weeks following surgery with complaints of pain in the left shoulder region. Plain chest radiograph demonstrated a well defined lytic lesion involving the head of the left humerus. Fine needle aspiration cytology of the left humeral head lesion rendered a diagnosis favouring squamous cell carcinomatous deposit. A further bone scan demonstrated increased radiotracer uptake in the left proximal humerus, trochanteric region of left femur and left fibula.
She was started on palliative radiation to the left humeral head and left fibula in view of pain relief. Palliative radiation was given till a dose of 30Gy in 10 fractions in 12 days with 3Gy per fraction. She was also started on palliative chemotherapy with three weekly Cisplatin and 5-Fluorouracil in view of systemic metastases and tumor cytoreduction. At last follow-up of six months following surgery, the patient was responding well to chemotherapy and was free of any bone pain.
DISCUSSION
Distant metastases outside the pelvis and abdomen may be seen rarely in vulvar malignancy. Vulvar carcinoma with bone metastases is an even rarer presentation.[3] Autopsies performed on 305 patients with gynaecological malignancies revealed four cases of asymptomatic bone metastases in patients with vulvar malignancies.[2] Bone scan is useful in detecting multiple bone metastases from vulvar cancer which can be confirmed immunohistochemically by the over expression of pan-cytokeratin MNF-116.[4] Palliative radiation therapy has been used in some cases for pain relief and tumor burden reduction.[3]
CONCLUSION
Bone metastases should be borne in mind in cases of unclear bone pains in women with gynaecological malignancies [4] and should be investigated properly. A plain radiograph is the most useful preliminary and cost-effective investigation in such cases and should be followed with a cytological or histopathological confirmation of the metastases. A bone scan will further supplement in delineating precisely the different sites of osseous metastases and to plan the treatment accordingly.
References:
- Brufman G, Krasnokuki D, Biran S. Metastatic bone involvement in gynaecological malignancies. Radiologica Clin. 1978;47:456-63.
- Abdul-Karim FW, Kida M, Wentz WB, Carter JR, Sorensen K, Macfee M et al. Bone Metastasis from Gynecologic Carcinomas: A clinicopathologic Study. Gynecol Oncol. 1990;39,108-14.
- Tolia M, Tsoukalas N, Platoni K, Dilvoi M, Pantelakos P, Kelekis N et al. Metastatic bone involvement in vulvar cancer: Report of a rare case and review of the literature. Eur J Gynaecol Oncol. 2012;33(4):411-13.
- Fischer F, Kuhl M, Feek U, Rominger M, Schipper ML, Hadji P et al. Bone metastases in vulvar cancer: a rare metastatic pattern. Int J Gynecol Cancer 2005;15:1173-76.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





