IJCRR - 9(2), January, 2017
Pages: 32-36
Date of Publication: 20-Jan-2017
Print Article
Download XML Download PDF
Ridge Augmentation Meet for Esthetics: An Interdisciplinary Approach
Author: Irudayanirmala J., Ramakrishnan T., Shobana P., Vidya Sekhar, Edilbert raja I., Karthikeyan A.
Category: Healthcare
Abstract:Aim: Dentoalveolar defects occur due to maxillofacial trauma, accidents, traumatic tooth extraction, advanced periodontal diseases, which results in loss of alveolar ridge and attached mucosa. These defects when occur in anterior region needs hard and soft tissue augmentation. Though many techniques exist for effective soft and hard tissue augmentation, approach is mainly based on the extent of the defect and specific procedures for prosthetic rehabilitation. Bone graft along with GBR is valuable treatment option for ridge augmentation followed by Fixed partial denture.
Case Report: This article presents case report of hard tissue augmentation in seibert`s class 3 alveolar ridge defect followed by Fixed partial denture with Gingival colored porcelain in missing Right maxillary lateral incisor region.
Discussion: Increase in the density of the defected area can be achieved by bone grafting with GBR. Thus it paves the way for replacement of the lost tooth along with function and esthetics.
Conclusion: The clinical and radiographic findings of this case suggests that bone grafting procedures combined with resorbable collagen membrane followed by esthetic metal ceramic fixed partial denture can be an acceptable alternative to removable partial denture, implant therapy.
Keywords: Dentoalveolar defects, Guided bone regeneration, Bioresorbable Demineralized bone matrix, Ridge augmentation, Fixed prosthesis
Full Text:
INTRODUCTION
Alveolar ridge augmentation designed to correct deformed alveolar ridge by enlarging or increasing, as in size, extent or quantity.1 Alveolar process is often affected after tooth loss by a continuous resorptive process in dentoalveolar defects. principal site of resorption is Labial aspect of the alveolar crest in which First reduces in width and later in height. These local alveolar ridge defects creates aesthetic and functional problems that includes loss of papillae, formation of open inter dental spaces, loss of buccal contour, unaesthetic gingival texture, phonetic problem, and food impaction respectively.2
Based on the location of the deformity, Seibert 1983 classified ridge defect as class1,class II, class III.2
Class 1 - Bucco lingual loss of tissue with normal apico coronal ridge height.
Class II – Apico coronal loss of tissue with normal buccolingual ridge width..
Class III - Combination of both buccolingual and apico coronal loss ( both width and height)
Advanced alveolar bone loss in above defects prevents replacement in an optimal prosthetic position. So ridge augmentation play a major role in replacement of teeth. It require bone regeneration outside of the existing bony walls that includes GBR techniques involving bone grafting material and membrane.3
GBR is technique that has same principle as GTR, but is not associated with teeth. Primary objective of GBR is to regenerate a single tissue i.e bone compared to GTR which regenerate multiple tissues (bone,cementum,PDL)4
Sterile bio resorbable Demineralized bone allograft has been used alone in ridge augmentation which is osteoconductive as well as osteoinductive in nature. GBR stabilize the bone graft below the membrane, minimize the risk of collapse and soft tissue in growth over osteogenic cells intended for bone regeneration.5
- This is the case report of Hard tissue augmentation with bone graft along with collagen membrane to enhance bone regeneration in seibert`s class 3 alveolar ridge defect in missing Right maxillary lateral incisor region. Later right maxillary lateral incisor was replaced with ceramic fixed partial denture with gingival-colored porcelain using central incisor and canine as abutments.
CASE REPORT:
- A 24 years old Female named Ramani was referred to the Department of periodontics, Adhi parasakthi dental college and hospital, for ridge augmentation, prior to fixed partial denture replacement by the Department of prosthodontics.
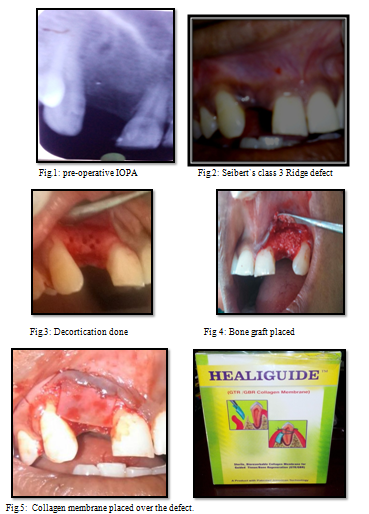
Implant was not planned because of inadequate width and height. Also patient needs immediate replacement. Medical history was Non-contributory. The dental history revealed, loss of Right maxillary lateral incisor due to trauma 1 year back. Evaluation of the edentulous space (through clinical and Radiographic examination) revealed siebert`s class 3 ridge defect (Combination of both buccolingual and apico coronal loss ( both width and height) [Fig.1,2] In order to create an emergence profile and soft tissue contour around the fixed partial denture, the ridge defect was planned to be corrected using Guided bone regeneration technique using bone graft with a resorbable collagen( Heali-guide) membrane.
SURGICAL CONSIDERATIONS:
RECIPIENT SITE:
Patient was asked to rinse with 10 ml of 0.2% chlorhexidine for one minute before surgery. Local anesthesia was given and crestal incision was placed on the edentulous area of Right maxillary lateral incisor region, continuing with the intra sulcular incision at the adjoining teeth.
Full thickness mucoperiosteal flap elevated that showed deformity in the labial aspect. A surgical bur was used to decorticate the bone for binding of bone graft over the defect area and also providing vascular supply.[Fig.3]
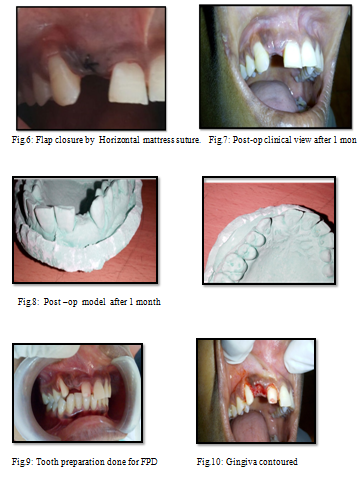
Allograft ( sterile bio resorbable Demineralized bone matrix- Xeno graft) was placed over the deformity[Fig.4] and covered with resorbable collagen membrane (HealiGuide).[Fig.5] Flap was closed by Horizontal mattress suture using 3-0 silk[Fig.6] and periodontal dressing was placed. Post operative instructions were given. Patient was advised Amoxicillin (500mg), three times daily for 5 days, and Ibuprofen (400mg) thrice daily or 3 days along with 10ml of chlorhexidine (0.2%) mouthwash twice daily for 14 days. The patient was recalled after 1 week for suture removal. Healing was satisfactory with no post surgical complications.
Patient was recalled after 1 month and clinical examination of the treated ridge defect showed significant improvement in ridge width.[Fig.7] Post operative models after 1 month showed improvement in ridge contour.[Fig.8]
RESTORATIVE PROCEDURE:
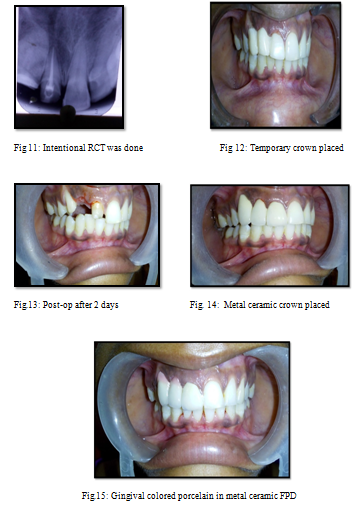
Teeth preparation done on maxillary central incisor and canine region.[Fig.9] Contouring of gingiva was done to get emergence profile[Fig.10] Since maxillary right central incisor pulp horn was so high, Intentional RCT was done on this tooth.[Fig.11].Immediately temporary crown placed.[Fig.12]. After 2 days post operatively, healing of gingiva took place with contoured margins. [Fig.13] In this case, young female patient had high esthetic expectations, Gingival-colored porcelain was used to metal-based ceramic crowns to compensate soft tissues on the maxilla .So metal ceramic crown with Gingival colored porcelain was constructed between maxillary right central incisor and canine region.[Fig.14,15] Then the prosthesis was checked for any occlusal discrepancies. The patient was instructed oral hygiene instructions including dental floss and interproximal brushes designed for fixed partial denture. The esthetic outcome of the procedure satisfied both clinician and patient.
DISCUSSION:
Large vertical and horizontal bone defects in missing teeth are not successfully treated by conventional fixed or removable prosthesis alone. Bone grafts with GBR showed successful bone regeneration in the ridge defects.
Bone regeneration occur at the periphery of the defect, by the formation of woven bone with new blood vasculature. New vascular supply comes from surgically created perforations in the cortical bone. Then woven bone is replaced by mature lamellar bone.4
Collagen membrane used for GBR has the ability to promote platelet aggregation, be chemotactic for fibroblast, enhance wound stability required for proper healing, and mechanical support to the tissue during bone formation.[5,6] Non –degradable membranes has been used for ridge defects with good results, however need of second surgery for its removal, and infection on exposure overcome by rersorbable membrane.
Recently, Non-expanded dense PTFE (Polytetrafluoroethylene) membrane provided sufficient regenerated ridge due to its no need for primary closure, easy to achieve over filling.7 Bone replacement grafts have an ability to stimulate progenitor cells .Progenitor cells undergo differentiation to osteoblasts and form bone under the membrane.5
There are various treatment options for the patients who have severe maxillary dento alveolar defects. Although removable partial dentures are indicated in soft and hard tissue lost in order to acquire lip support. They are not the first choice of patients who have high esthetic and functional expectations.
Conventional tooth supported FPD may be an ideal treatment option where implants are contra indicated or patients refuse the implant therapy due to its surgery, and long time to complete the treatment. However, Natural abutment teeth with sufficient bone support are required for these kinds of prosthesis. Moreover it reduces treatment time and cost.8
CONCLUSION:
- Prior to treat Dentoalveolar defects, Careful diagnosis and surgical – prosthetic treatment planning with joint consultation should be performed. In order to obtain better results, ridge augmentation with bone grafting along with GBR is more predictable and metal ceramic fixed partial denture with Gingival-colored porcelain enhanced the esthetic outcome. Correction of a localized ridge defect with hard tissue augmentation is a valuable method for FPD in which improved mucogingival esthetics as well as phonetics.
ACKNOWLEDGEMENT:
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
- American Academy of Periodontology. Glossary of periodontal Terms (2001).
- Lakshmaiahenkatesh P.M, Suryaprakash M.S, Varadan K.B, Rajanna.S. Pre psosthetic reconstruction of alveolar ridge. Journal of the International clinical Dental Research organization, 2011; 3(2) : 78-83.
- Aparna singh, Anika Daing, Vishal Anand. Two dimensional alveolar ridge augmentation using particulate hydroxy apatite and collagen membrane: A Case report. Journal of oral biology and cranio facial research, 2014;4:151-4.
- Newman MG, Takei HH, Klokkevold PR, Carranza FA. Caranza`s clinical periodontology.10th ed. St.Louis: Elsevier (saunder`s);2006.p.113
- Parthasaradhi T, Preethe Padmanabhan, Ramya V. Successful localized ridge augmentation: A combination therapy using GBR and PRP. Biomedical andPharmacology Journal,2015;8:347-52.
- Rakhmatia Y.D, Ayukawa Y, Furuhashi A, Koyano K. Current barrier membranes: Titanium mesh and other membranes for guided bone regeneration in dental applications. Journal of prosthodontic research,2013;57:3-14.
- Yamashita M, Horita S, Takei N, Sasada Y. Minimally invasive Alveolar ridge preservation /Augmentation procedure. Funakoshi Research institute of clinical periodontology.
- Yazicioglu Y, Ozkurt-Kayahan Z, Ozcakir-Tomruk C, Katipoglu B. Prosthetic management of a Maxillary Alveolar defect with an Implant-Retained Fixed prosthesis: A clinical report. Dentistry,4(5):225.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





