IJCRR - 5(23), December, 2013
Pages: 06-09
Date of Publication: 16-Dec-2013
Print Article
Download XML Download PDF
VARIATION IN THE ORIGIN OF LEFT VERTEBRAL ARTERY WITH INCREASE IN THE LENGTH OF BRACHIOCEPHALIC TRUNK
Author: Gavishiddappa A. Hadimani, Ishwar B. Bagoji, B. M. Bannur, R. S. Bulagouda, B. G. Patil, Sahana B. N.
Category: Healthcare
Abstract:An understanding of the variability of vertebral artery remains most important in angiography and surgical procedures where an incompatible knowledge of anatomy can lead to complications. Vertebral artery is important artery to supply posterior part of cerebral circulation. During routine dissection of cadaver for undergraduate dissection we encountered variations in relation to origin of left vertebral artery. Variant left vertebral artery was arising from arch of aorta directly. In the right side of the same cadaver length of vertebral artery was reduced due to increase in the length of brachiocephalic trunk.
Keywords: Arch of aorta, Brachiocephalic trunk, Cervical vertebra, Vertebral artery
Full Text:
INTRODUCTION
The vertebral artery is important artery to supply posterior part of cerebral circulation. According to the standard textbooks of anatomy, vertebral artery is the largest and constant stem of subclavian artery, both in origin and distribution. It arises from the superior surface of the first part of the subclavian artery medial to the scalenus anterior muscle. The vessel takes a vertical posterior course to enter into the transverse process of the sixth cervical vertebra. It continues through the transverse foramina of the cervical vertebrae and after passing through the transverse foramen of the atlas, turns posteromedially on its posterior arch, pierces the atlantooccipital membrane and the dura mater, respectively and then enters the foramen magnum [1]. Both Vertebral arteries unite at the caudal border of the pons to form unpaired basilar artery. This vessel courses along the ventral aspect of the brainstem [2, 3]. The segment of the vertebral artery from its origin at the subclavian artery to its entry into the respective transverse foramina is called the pretransverse or prevertebral segment [4].
An understanding of the variability of vertebral artery remains most important in angiography and surgical procedures where an incompatible knowledge of anatomy can lead to complications [5].
CASE REPORT
During routine cadaveric dissection for undergraduate students in the department of anatomy Shri B M Patil Medical College, Hospital and Research centre, BLDE University, Bijapur we found variation in the origin of left vertebral artery and length of brachiocephalic trunk on right side was increased, the details are explained below. Variations were dissected, examined and photographed. Variations include,
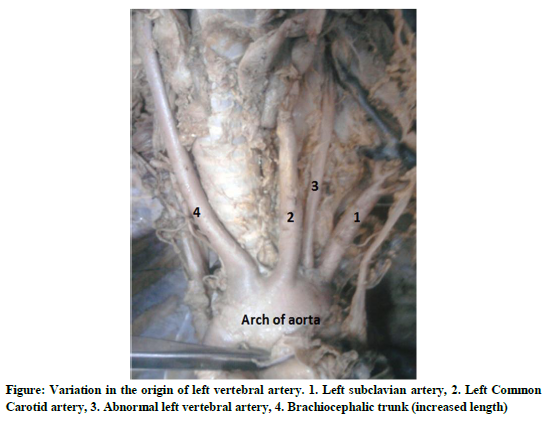
Variation in the origin of left vertebral artery: left vertebral artery originated directly from arch of aorta between the origin of left common carotid artery and left subclavian artery. The distance between the origin of left vertebral artery and
neighboring arteries were 3 mm and 4 mm respectively. Diameter of the left vertebral artery at its origin was 6 mm. The variant left vertebral artery coursed upward to the transverse foramen of the 6th cervical vertebra. The length of the prevertebral segment of the variant left vertebral artery was 93 mm. (fig -1)
Increase in the length of brachiocephalic trunk: The length of the brachiocephalic trunk was increased to 74 mm, undue increase in the length of the brachiocephalic trunk is noticeable. After its prolonged course upwards brachiocephalic trunk divided in to right subclavian and right common carotid artery. The right vertebral artery originated from the right subclavian artery like normal right vertebral artery. The right vertebral artery entered the transverse foramen of the 6th cervical vertebra. The length of the prevertebral segment of the right vertebral artery was 23 mm (fig -1).
DISCUSSION
The vertebral artery is subject to mechanical stress, dynamic obstructions, thrombosis that propagates to brain infarction and traumatic dissecting aneurysms in addition to constriction, embolism, and occlusive disease. Pathology of the vertebral artery is characterized by catastrophic strokes in the young and by disability without stroke.
Anatomical variations in the major vessels of have been reported earlier. The review of literature shows many variations. It is very common to find the variation in the origin of left vertebral artery especially from arch of aorta, but it is not common to find the increased length of brachiocephalic
trunk. However, increased length of brachiocephalic trunk has not been reported to the best of our knowledge.
The left vertebral artery may arise directly from left common carotid artery, left subclavian artery or from arch of aorta. The frequency of left vertebral artery arising from arch of aorta in Japanese study was 5.8%. There was no difference between male and female [6]. In the Indian study 1.6% had left vertebral artery as branch of arch of aorta. Five out of six cadavers with the anomalous aortic arch branching were females. One male cadaver presented an anomalous origin of left vertebral directly from arch [7].
A study by poonam et al left vertebral artery originated from the external carotid artery in common with occipital artery at the level of intervertebral disc between C2 and C3 vertebrae and took the course without entering any foramen transversarium [8].
Lippert Pab’s classified the left vertebral artery according to the origin from the aortic arch as Type A, B, C, D, E, F, G and H, left vertebral artery between the left common carotid artery and left subclavian artery as Type A(3%), between a common trunk formed by brachiocephalic trunk and left common carotid artery and left subclavian artery as Type B(<1%), after the left subclavian artery as Type C(<1%), after the left subclavian artery as the third branch as Type D(<0,1%), after a common trunk as the second branch as Type E(<0,1%), different from Type A, right subclavian artery appears from descending aorta as Type F(<0,1%), one of two roots as a penultimate branch as Type G(<1%), both vertebral artery branch from the aortic arch as Type H(<0,1%) [9].
EMBRYOGENESIS
Usually the first part of vertebral artery develops from proximal part of dorsal branch of seventh cervical intersegmental artery proximal to postcostal anastomosis. The second part is derived from longitudinal communications of the postcostal anastomosis with the consequent regression of the stems of the upper six intersegmental arteries. Third part develops from spinal branch of the first cervical intersegmental artery. Fourth part owes its development from the pre neural division of the spinal branch [1].
Arey is of the view that the anomalous blood vessels may be due to (i) the choice of unusual paths in the primitive vascular plexus, (ii) the persistence of vessels normally obliterated, (iii) the disappearance of vessels normally retained, (iv) incomplete development, and (v) fusions and absorption of the parts usually distinct [10].
In the left side left sixth dorsal intersegmental artery might have persisted as the first part of vertebral artery hence left vertebral artery was arising from arch of aorta, but on the right side right limb of aortic sac might have increased in length. Progressive development on the right side may be to meet the nutritional demand by the upper limb, head, neck and brain.
CONCLUSION
Understanding of the variability of vertebral artery becomes most important in angiography and surgical procedures. Incompatible knowledge of anatomy may lead to complications. Major branches of arch of aorta are ways for blood supply to the head and upper limb, and are of particular interest in clinical angiography. The proximal parts of these branches are common sites for atherosclerosis with clinical consequences for blood supply to brain. Abnormalities of these branches can cause changes in cerebral hemodynamic that may lead to cerebral abnormalities.
References:
- Moore KL. The Developing Human. Clinically Oriented Embryology. 3rd Ed. WB Saunders, Philadelphia. 1982; 291–318.
- Clemente CD. Anatomy–A Regional Atlas of Human Structure. 4th Ed., Baltimore- Philadelphia-London-Paris-Bangkok-Buenos Aires-Hing Kong-Munich-Sydney-Tokyo-Wroclaw, Williams and Wilkins. 1997; 458–459.
- Drake RL, Vogl AW, Mitchell AWM. Gray’s Anatomy for Students. 2nd Ed., Edinburg-London-Melbourne-New York, Churchill Livingstone. 2005; 976.
- Matula C, Trattnig S, Tschabitscher M, Day JD, Koos WT. The course of the prevertebral segment of the vertebral artery: anatomy and clinical significance. Surg Neurol. 1997; 48: 125–131.
- Wasserman BA, Milkulis DJ, Mananzione JV. Origin of the right vertebral artery from the left side of the aortic arch proximal to the origin of the left subclavian artery. AJNR Am J Neuroradiol. 1992; 13: 355–358.
- Koh-ichi. Yenke et. Al anatomical study of vertebral Japanese adults. Anatomical science International; 2006: 81, 100-6
- Nayak SR, Pai MM, Prabhu LV, D’Costa S, Shetty P. Anatomical organization of aortic arch variations in India: embryological basis and review. J Vasc Bras 2006; 5:95-100.
- Poonam , Singla R K , Sharma T . Incidence of anomalous origins of vertebral Artery - anatomical study and clinical significance. J of Cli and Diagnostic Research: 2010; 4:2626-31
- Lippert H, Pabst R. Arterial Variations in Man. Classification and Frequency. JF Bergmann Verlag, Munchen. 1985; 30–38.
- Arey LB. Development of arteries. The vascular system In Developmental Anatomy. A Textbook and Laboratory Manual of Embryology. 6th Ed., Philadelphia and London, WB Saunders Company. 1957; 367–373.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





