IJCRR - 5(23), December, 2013
Pages: 01-05
Date of Publication: 16-Dec-2013
Print Article
Download XML Download PDF
ASSOCIATION BETWEEN FUNCTIONAL REACH TEST AND STAR EXCURSION BALANCE TEST IN HEALTHY CHILDREN OF 14-16 YRS
Author: Atiya A. Shaikh, Radhika Walunjkar
Category: Healthcare
Abstract:Objective: To score and correlate Functional reach test distance and star excursion balance test distance in children between 12-16 years. Material and Method: 200 healthy children were assessed using Functional reach test and star excursion balance test. Results: Pearson's correlation showed very strong positive to strong positive association between scores of Functional reach test and Star excursion balance test (in all directions). Conclusion: Functional Reach Test and Star Excursion Balance Test can be used interchangeably to assess dynamic balance in children.
Keywords: dynamic balance strategies, feed Functional mechanism, children, Functional reach test, star excursion balance test.
Full Text:
INTRODUCTION
Balance assessment is necessary for many patients in physiotherapy setting in order to establish appropriate treatment goals, reduce fall risk, increase awareness for appropriate device and treatment prescription, designing of fall prevention programs and prognosis assessment1.
An individual has to perform multiple tasks that challenge dynamic postural control system to perform ADL’s effectively. For the balance assessment to be accurate, the test used should attempt to simulate conditions of day to day life in order to stress postural control system to its maximum limit2. Keeping this in mind, the clinicians should use functional tasks performed in day to day life to assess balance in clinical set up. These tasks are also should be chosen according to their familiarity with the subject, lesser time and resource consumption1,2.
A child develops adult like balance by the age of seven years3. Common functional activities performed by them include reaching in various directions with upper limb and lower limb with in and out of base of support, running and jumping. Scales like Berg balance scale, Bruinnik’s Osterestky test of motor proficiency, balance efficacy scale simulate these activities4 but require more time, space and few equipments hence it is unsuitable for busy clinical setting.
The activities mentioned in above scales are mimicked by functional reach test and star excursion balance test6, 7.
Functional reach test assesses the distance a person can reach in front beyond arm’s length while maintaining fixed base of support in standing position6. Ankle strategy of postural control is challenged in this test where as Star Excursion Balance Test involves moving in
prescribed directions while maintaining balance on contra lateral leg7. The person relies on stepping strategy of postural control for maintaining balance effectively in this test.
Functional reach test has been used traditionally to assess dynamic balance in healthy and patient population of all ages 6,8,9 where as star excursion balance test is gaining popularity as dynamic assessment tool for healthy and sports person of young and elderly 7,10,11,12,13. These two tests can be preferred for healthy children due to their familiarity with the functional activities of children.
Validity of functional reach test for children of 14-16 yrs is proved8 but the same for Star excursion balance test for this age group is yet to be established. As both these tests involve use of feed forward postural control strategies, they may be inter related. A positive association between these two tests will ensure the validity of star excursion balance test for this age group. In that case, any one of these tests can be used instead of two to evaluate balance for all related dynamic activities thus reducing evaluation time.
The co-relation between these two tests and their usefulness to assess dynamic balance in 14-16 yrs of children is still unexplored. Thus this study was designed to find the association between FRT and SEBT in children between 14-16 yrs.
MATERIALS AND METHODS
Research Design: Cross sectional
Inclusion Criteria
Healthy children of both genders between age group of 14 yrs to 16 yrs
Exclusion Criteria
Children with Mental retardation, known behavioural, cognitive, sensory, vestibular, musculoskeletal or neuromuscular disorders
Setting of the study
Public schools in Pune
Sample size
200 children
Sample Selection Method
Convenience
Materials Used
Measuring tape, chalk, Score sheets
PROCEDURE
Ethical committee clearance from college authorities and consents from the school authorities and parents were obtained. Children were assessed using Functional reach test and Star excursion balance test using standardized procedures6,7. Findings were noted and analysed using SPSS11.00 version.
OBSERVATION AND RESULTS
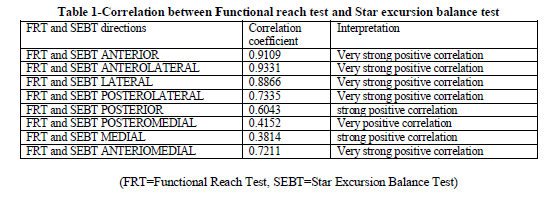
Pearson’s correlation coefficient value for FRT and SEBT in anterior, anterolateral, lateral posterolateral, posterior, posteromedial, medial, anteromedial direction was 0.9109, 0.933, 0.8866, 0.7335, 0.6043, 0.4152, 0.3814, 0.7211.
DISCUSSION
An individual has to perform a varied range of activities in order to complete ADL’s effectively and independently. These different tasks challenge postural control system in different ways and directions thus involving use of feedback, feed forward mechanisms and ankle, hip, or stepping strategies. Appropriate mechanism is chosen according to task being preformed14.
Change in task causes movement of different body segments, alters anticipatory postural adjustments and results in inclusion of other uninvolved segments for stabilising body those body thus altering the muscle activation sequence. The postural control mechanism involved may be same for different activities but, the muscle activation sequence while performing those activities will change according to the part moved out of base of support and parts required to stabilise the body while this task is being performed14.
Activities preformed by children like reaching for objects in different directions or playing, involve variation of centre of gravity in different directions
with in and out of base of support thus a varied activation of muscles involved in anticipation to the movement. FRT involves reaching in front as far as possible keeping foot in complete contact with ground. This task causes displacement of centre of gravity in forward direction by rotating around ankle joint with maintained hip extension thus activating ankle or hip strategy. It has been observed that healthy individual use ankle strategy to perform such tasks. Here, the gastro-soleus are the main muscle activated along with other anti gravity muscles required for a closed chain activity15.
The other commonly performed action by children while playing is running and jumping .These are dynamic activities causing stepping response in relation to the continuously changing base of support and centre of gravity. Test like SEBT is reaching as far as possible with one leg in each of eight directions while maintaining balance on contra-lateral limb. Here, the standing leg requires, good range of motion of ankle dorsiflexion, knee flexion, hip flexion, adequate Glutei and other antigravity muscle strength in order to control closed kinematic motion occurring while performing the task. As this task involves use of antero - posterior and medio-lateral feed forward postural strategies, it challenges gluteus maximus, medius, minimus, gastro-soleus and tibialis anterior both. The feed forward postural control mechanism along with different muscle activation and strategies is challenged while reaching in anterior, anteromedial, anterolateral, medial, lateral, postero-medial, postero-lateral and posterior direction to complete the test12.
FRT and SEBT both challenge feed forward postural responses but the sequencing of stabilisation forces and activation of muscles required and strategy being used while performing these tests is different .12,15
This study shows that, there is a very strong positive co-relation between FRT and SEBT scores of anterior, anterolateral, posterolateral lateral, anteromedial direction whereas, strong positive correlation between FRT and SEBT scores of posterior and medial direction and positive correlation between FRT and SEBT posteromedial direction scores in children between 14-16 yrs. This finding proves the hypothesis that, both tests are associated as the underlying mechanism for postural control is same. It also validates SEBT as a tool for dynamic balance assessment. This can help the therapists to choose appropriate test to assess dynamic balance as per the need of assessment and condition of the subject to be assessed. The patients with upper extremity affection can be judged by their SEBT skills and the patients with lower limb impairment can be judged by their FRT skills for their dynamic balance.
We know that, height and weight are found to influence FRT and SEBT distance12,9 but, since this study was performed to compare distances of same children these factors were not considered. It has been proved that gender does not affect the distance reached in both tests hence children of both gender were included as per the availability of them.
The main limitation of the study is sample selection by convenience sampling method ,a larger sample size with random sampling method would have been more appropriate for generalising the observations of this study.
CONCLUSION
FRT has been used as a valid assessment tool for balance evaluation since a long time .The study proved a positive correlation between both the tests, thus it highlights the validity of SEBT in this age group. As SEBT requires no equipment and is a preferred activity in children it should be used widely to assess balance in this age group. They can be used interchangeably to assess dynamic balance in children. Any one of these tests can be used instead of two to evaluate balance for all related dynamic activities thus reducing evaluation time.
ACKNOWLEDGEMENT
We would like to thank students, parents and principals of all schools visited, along with Dr. Sujit Kadrekar, Dr. Aparna Sadhale (PT), Dr Rashmi Joshi (PT), Dr. Abha Dhupkar (PT), for their support and encouragement. We acknowledge the great help received from scholars whose articles cited and included in references of this manuscript. We are grateful to authors, editors and publishers of all those articles, journals and books from where the literature of this article has been reviewed and discussed. We are also grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
- Browne J, O'Hare N. A Review of the Different Methods for Assessing Standing Balance. Physiotherapy. 2001. 87; 9:9489-495.
- Furman J .Posturography: Uses and Limitations. Balliere’s Clinical Neurology.1993;3: 501-513
- Shumway –Cook A, Woollacott M:translating research into clinical practice; Motor control posture and balance, Development of posture and balance ,ed-4.Lippincott Williams and Willkins,United states,2011;162,221-222
- Alexandra K, Inge D, Wim P et al. Construct Validity of the Assessment of Balance in Children Who Are Developing Typically and in Children With Hearing Impairments
Physical therapy 2010; 90: 1783-1794
- Kembhavi G, Darrah J, Magill-Evans J, Loomis J. Using the Berg Balance Scale to distinguish balance abilities in children with cerebral palsy. Pediatr Phys Ther. 2002;14:92–99
- Donahoe B, Turner D, Worrel T. The use of functional reach as a measure of balance in boys and girls without disabilities of age 5-15 yrs. Pediatric Physical therapy 1994;6:189-193
- Gribble P A. The star excursion balance test as a measurement tool. Athl. Ther Today 2003;8(2):46-47
- Bartlett D, Birmingham T. Validity and reliability of pediatric reach test .Pediatric Physical therapy 2003;15:84-92
- Volkman K, Stregious N ,Stuberg W et al. Methods to improve the reliability of functional reach test in children and adolescents with typical development. Pediatric physical therapy.2007;19:20-27
- Robinson RH, Gribble PA,Support for reduction in number of trials needed for SEBT Archives of physical medicine and rehab. 2008.89(2); 364-370
- Kinzey S, Armstrong C. The reliability of the Star-Excursion Tests in assessing dynamic balance. J Orthop Sports Phys Ther. 1998; 27:356-360.
- Lauren C, Olmsted, Christopher R, et al. Efficacy of SEBT in detecting reach deficits in subjects with chronic ankle instability. J Athl.Train.2002;37(4):501-506
- Gribble PA, Hertel J, Plisky P. Using the Star Excursion Balance Test to Assess Dynamic Postural-Control Deficits and Outcomes in Lower Extremity Injury: A Literature and Systematic Review, Journal of athletic training 2012; 47(3): 339-357
- Winter D.Human balance and posture control during standing and walking .Gait and Posture;1995;Vol.3:193-214
- Wernick-Robinson M, Krebs DE, Giorgetti MM. Functional reach: does it really measure dynamic balance? Arch Phys Med Rehabil. 1999;80:262–269
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





