IJCRR - 5(24), December, 2013
Pages: 61-63
Date of Publication: 31-Dec-2013
Print Article
Download XML Download PDF
PHAEOHYPHOMYCOSIS - A RARE INFECTION WITH TWO DIFFERENT CLINICAL PRESENTATION
Author: Volga Harikrishnan, Sonti Sulochana, Meenakshi Sundaram, Aruna Gnanaguruparan, Chitra Srinivasan
Category: Healthcare
Abstract:Phaeohyphomycosis is rare mycotic infections caused by melanized fungi. We report two cases of phaeohyphomycosis with different clinical scenario but with typical similar histopathological features.
Keywords: phaeohyphomycosis, melanised fungi
Full Text:
INTRODUCTION
Phaeohyphomycosis is caused by ubiquitous fungai and it can occur in any forms like septate hyphae, pseudohyphae, and yeast forms in tissue. Clinical manifestations of the disease range from localized superficial infections of the stratum corneum to subcutaneous cysts (phaeomycotic cyst) to invasion of the brain.
CASE REPORT
Case 1
A 70 year old male presented with swelling in the dorsum of right little finger for 2 months duration. The lesion was associated with pain which was intermittent and pricking type. History of trauma (Thorn injury) was present. He was non- diabetic and had no other systemic or underlying disease. Clinically the case diagnosed as sebaceous cyst.
Case 2
An immunodeficient, 50 year old female presented with swelling in the left hand for 3 weaks duration. The lesion was not associated with pain. No history of trauma present. She was diabetic for the past 15 years.
PATHOLOGICAL FINDINGS
Gross features
Both cases showed typical similar gross features. No contents were present. Inner surface of the cyst was brownish, case 1 showed fine nodularity in addition. Wall showed whitish and yellowish areas.
Microscopic features:
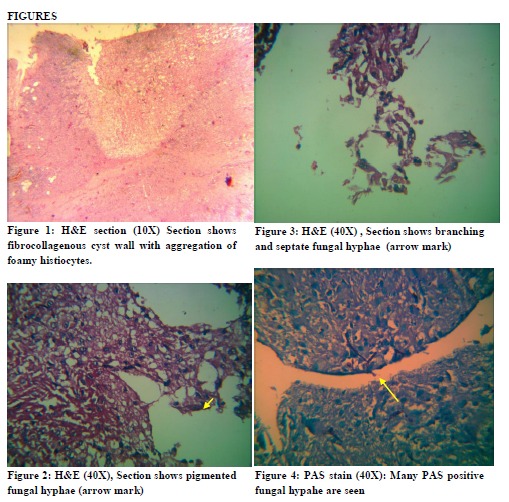
Sections from both cases showed fibrocollagenous cyst (Fig 1) wall lined by granulomas composed of epitheliod cells, foreign body and Langhan giant cells. The wall contains aggregates of foamy histiocytes, mixed inflammatory cell infiltrate and necrosis. Pigmented and branching fungal hyphae (Fig 2 &3) seen.
We did Periodic acid schiff (PAS) stain for both cases which showed branching and septate fungal hyphae morphologically consistent with Phaeohyphomycetes (Fig 4).
Ziehl-Nielsen staining was done for acid fast bacilli and it was negative for tubercle bacilli
DISCUSSION
The dematiaceous (brown-pigmented) fungi are heterogenous group of moulds that cause a wide range of diseases including phaeohyphomycosis, chromoblastomycosis and eumycotic mycetoma (1).
Phaeohyphomycosis, is a rare infection, although the number of cases has been increasing in recent years (2). These fungi are found in soil, wood and plant as saprophytes. The presence of melanin in their cell walls may be a virulence factor for these fungi (3).
Typically, phaeohyphomycosis follows traumatic implantation (4) of the fungus by a wooden splinter, as in one of our case. The primary risk factor is decreased host immunity, although cases in apparently immunocompetent patients (5) have been reported.
The spectrum of the disease includes superficial, cutaneous, subcutaneous and systemic infection (6).
Etiologic agents include Exophiala, Phoma, Bipolaris, Phialophora, Colletotrichum, Curvularia, Alternaria, Exserohilum, and Phialemonium sp (7).
Rarely it can cause fatal disease as reported by (8) .He reported a case of cerebral phaehyphomycosis in a patient with neurosarcoidosis with the history of marijuana smoking and chronic steroid therapy.
The common manifestations clinically are cystic lesions as seen in our cases or abscesses (9).
Most forms of disease caused by dematiaceous fungi require both medical and surgical treatment. The most effective antifungal agent for subcutaneous phaeohyphomycosis is Itraconazole. Complete surgical resection can also be done for discrete lesions (1).
CONCLUSION
Since it is a rare fungal infection, the incidence has been increasing irrespective of immune status of the patient. We have presented two case reports with different clinical presentation one in immunocompetent individual, with trauma history and another one, immunodeficient patient without any triggering factor. Histopathological examination of tissue section along with special stain plays an important role in the diagnosis of Phaeohyphomycosis.
References:
- Brandt ME ,Warnock DW. Epidemiology, clinical manifestations, and therapy of infections caused by dematiaceous fungi. J Chemother. 2003 Nov; 15 Suppl 2:36-47.
- Vasquez-del-Mercado et al. Subcutaneous phaehyphomycosis due to Curvularia lunata in renal transplant patient.Rev Iberoam Micol.2013 Apr-Jun;30(2):116-8
- Sanjay G. Revankar, Jan E. Patterson, Deanna A. Sutton, Disseminated Phaeohyphomycosis:Review of an Emerging Mycosis, Clinical Infectious Diseases 2002; 34:467–76.
- Madhavan Manoharan, Natarajan Shanmugam, Saveetha Veeriyan. A Rare Case of a Subcutaneous Phaeomycotic Cyst with a Brief Review of Literature. Malaysian J Med Sci. Apr-Jun 2011; 18(2): 80-83.
- Devesh Mishra, Maneesh Singal, Mahaveer Singh Rodha. Subcutaneous Phaeohyphomycosis of Foot in an Immunocompetent Host. J Lab Physicians, 2011 Jul; 3(2):122-4. doi: 10.4103/0974-2727.86848
- McGinnis MR, Chromoblastomycosis and phhaehyphomycosis: new concepts, diagnosis, and mycology. J Am Acad Dermatol.1983 Jan; 8(1):1-16.
- Isa-Isa R, Garcia C, Isa M, Arenas R. Subcutaneous phaeohyphomycosis (mycotic cyst). Clin Dermatol. 2012 Jul-Aug; 30(4):425-31.
- Gongidi P et al. Cerebral phaehyphomycosis in a patient with neurosarcoidosis on chronic steroid therapy secondary to recreational marijuana usage, Case Rep Radiol.2013; 2013:191375.
- Yoon Ya et al. Subcutaneous phaehyphomycosis caused by Exophiala salmonis. Ann Lab Med.2012 Nov; 32(6); 438-41.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





