IJCRR - 6(23), December, 2014
Pages: 01-09
Date of Publication: 10-Dec-2014
Print Article
Download XML Download PDF
UNILATERAL QUADRIFURCATION OF RENAL ARTERY: A RARE VARIATION AND ITS CLINICAL IMPLICATIONS
Author: Bharambe V. K., Shinde A. A.
Category: Healthcare
Abstract:Introduction: Renal transplantation has become the treatment of choice for most patients with end-stage renal disease. This involves recovering the kidney along with adequate vessel length from the donor and implanting it into the recipient anastomosing all vessels diligently. Usually \"single renal artery kidneys\" are preferred. However with the ever increasing waiting list of patients needing kidney transplants, kidneys with multiple arteries supplying it, are also used for transplant purposes. Case study: During routine dissection of an adult male cadaver by medical students, the aorta and right renal artery showed variations. Result: The right renal artery was observed to be quadrifurcating into inferior phrenic, inferior suprarenal and two duplicate renal arteries. There was no middle suprarenal artery and the branches of renal artery or their branches were the sole arterial supply to the suprarenal gland. No variations were observed in the branching pattern of the left renal artery. Discussion: Precise knowledge of renal arterial supply and associated variations is critical for success of renal surgeries as well as to avoid complications. Present article discusses the details of the rare hitherto unreported variation of \"quadrifurcation of renal artery\", its possible embryological explanation and its clinical implications from point of view of renal surgeries.
Keywords: Renal Artery, inferior phrenic artery, inferior suprarenal artery, quadrifurcation of renal artery, duplication of renal artery
Full Text:
INTRODUCTION
With advent of science, kidney transplantation is almost considered a common surgery today. It involves removal of kidney from the donor and implanting it into the recipient anastomosing every vessel with the recipient’s vessels. The knowledge of vessels supplying the kidney, its surrounding structures and possible variations in these vessels therefore is of paramount importance for the operating surgeon. Many researchers have reported various variations in origin, number and branching pattern of the renal arteries (1,2). There have also been reports of variations in origins and branching patterns of both suprarenal and inferior phrenic arteries.(3,4) However there are no reports of variations of all the above mentioned arteries being observed in the same individual as in the present case where we report finding of “quadrifurcation” of right renal artery into inferior phrenic artery , inferior suprarenal artery and 2 duplicate renal arteries.
CASE STUDY
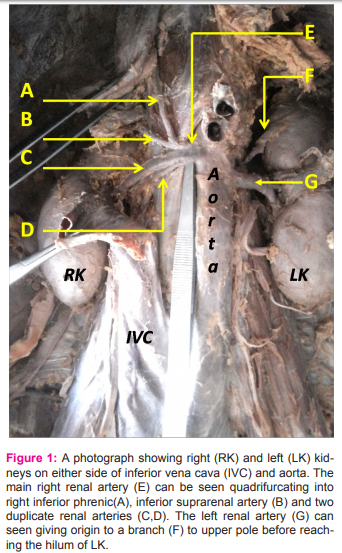
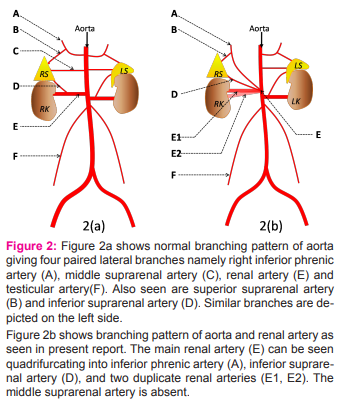
During routine dissection of a 40 year old male cadaver preserved in 10% formalin, by medical students, it was found to be showing a variation in the branching pattern of aorta and of the right renal artery. The right renal artery was observed to be taking origin from aorta slightly below the origin of superior mesenteric artery. (Fig 1,2a,2b) This was referred to as the main right renal artery. The trunk of the main right renal artery was resting posteriorly on the right crus of diaphragm, covered anteriorly by Inferior vena cava. It was about 6 mm long and quadrifurcated into four branches namely inferior phrenic artery, inferior suprarenal artery and two duplicate renal arteries of the right side. On further dissection the inferior phrenic artery was seen giving rise to a small superior suprarenal artery which along with the inferior suprarenal artery, supplied the right suprarenal gland. The right middle suprarenal artery was absent. The two duplicate renal arteries gave rise to multiple branches that supplied the kidney. The duplicate renal arteries were situated such that one was anteriorly placed and the other posterior to it. The left renal artery took origin from aorta at a slightly lower level compared to right renal artery and immediately gave rise to a branch which supplied the region of upper pole of left kidney as well as the left suprarenal gland. The rest of left renal artery divided into branches at the hilum of left kidney to supply it. It also gave origin to the left inferior suprarenal artery. The left inferior phrenic artery and middle suprarenal artery were observed to be direct branches of aorta.
DISCUSSION
The abdominal aorta gives rise to inferior phrenic arteries at the level of T12.(Fig 2a,b) These are a pair of parietal branches that supply the diaphragm. It also gives rise to middle suprarenal arteries and renal arteries at a lower level, which are pairs of visceral arteries supplying suprarenal glands and kidneys respectively. The inferior phrenic arteries and renal arteries give origin to superior and inferior suprarenal arteries respectively, which supply the suprarenal gland along with the middle suprarenal artery(5). Renal arteries are two large vessels, branching laterally from the aorta, just below superior mesenteric artery. These are end arteries with no anastomoses. The right renal artery is longer than left, passes behind the inferior vena cava and right renal vein. Near the hilum each renal artery divides into three to four branches which lie mostly between the renal vein anteriorly and the ureter posteriorly but some branches may lie posterior to the hilum of kidney. One or two accessory renal arteries are frequently seen especially on the left side(6). There have been many reports of accessory renal arteries. Rao and Rachana in 2011 have described a unilateral right sided accessory renal artery that arose separately from the aorta to supply the upper pole of right kidney(7). Shinde et al reported finding of an unilateral accessory inferior hilar artery in a case of tortuous abdominal aorta(8). Shinde and Bharambe give a 4% incidence of lower polar supernumerary renal artery(9). Kanaskar et al have described two accessory renal arteries on the right side, one of which arose from aorta while the other was a branch of renal artery (2). Mehta and Arole have described finding of 11 cases of accessory renal arteries out of 50 kidneys studied (10). However finding of duplicate renal arteries is rare. Patel et al described a case of unilateral left sided double renal artery, one of which arose from aorta at L1 level while the other arose 5 cm below it(11). Budhiraja et al have reported 8.33% incidence of finding of duplication of renal arteries with a higher incidence on the right side compared to left (1). These duplicate renal arteries were situated anteriorly and posteriorly emerging at the same level from aorta. The present article reports duplicate renal arteries with a similar disposition (Fig 2b). Such duplicate hilar arteries have also been referred to as double hilar arteries. Triple hilar arteries have also been described, but were not observed in present case (12). Bergman reported that the middle suprarenal artery can be found to be replaced by the superior suprarenal artery (3). More often it can be replaced by the inferior suprarenal artery. In present case the superior suprarenal artery was found to be a branch of inferior phrenic artery which was a branch of renal artery, the middle suprarenal artery was absent and the inferior suprarenal artery arose from the renal artery (fig 2b). Thus the middle suprarenal artery was replaced by the inferior suprarenal artery. Topaz et al have described finding of a common trunk of inferior phrenic arteries taking origin from right renal artery and then diving into the right and left inferior phrenic arteries (4). In the present study it was observed that while the right inferior phrenic artery arose from the right renal artery, the left inferior phrenic artery was a direct branch of abdominal aorta (Fig 2b). Both the inferior phrenic arteries in turn gave origin to the superior suprarenal artery which supplied the right and left suprarenal glands respectively. Associated with variations in renal arteries, there are also reports of variations in origin of testicular arteries. Panagouli et al have described a case where there was bilateral origin of testicular arteries from accessory renal arteries (13). In present case however the testicular arteries were both taking origin directly from abdominal aorta (Fig 2b). Thus parts of various observations found in the present study have been reported earlier, however finding many of the variations together in one cadaver, in the form of quadrifurcation of the main right renal artery branching into inferior suprarenal artery, inferior phrenic artery and two duplicate renal arteries is hitherto unreported. Embryological explanation for the present variation has been discussed by Keibel (14). He stated that the developing mesonephros, metanephros, suprarenal gland and the gonads are all supplied by nine pairs of lateral mesonephric arteries arising from aorta. He divided these arteries into three groups as cranial, middle and caudal arteries. The middle group gives rise to renal arteries and if one extra artery persists partly, it results in formation of duplication of renal artery. A possible fusion of point of origin of cranial and middle lateral mesonephric arteries of right side could explain the quadrifurcation seen in present case report. The anatomical knowledge of existence of multiple arteries or arterial variations is essential before performing any transplantation surgeries where microvascular techniques are employed to reconstruct the renal arteries (15). Transplanting a kidney with renal arterial variation has the disadvantage of higher chances of acute tubular necrosis and graft rejection, as well as decreased graft function and hence transplantation of kidney with single renal artery is preferred (16). But because of increasing demand for kidney transplantation, transplanting kidneys with multiple arteries has become necessary. Also recent advances in technology of microvascular surgery have enabled dependable reconstruction of multiple renal vessels in donor kidneys (15). In these circumstances in order to know the vascular pattern and to plan the surgery, computer tomography and renal angiography should be performed prior to every urological procedure (16). The knowledge of renal vascular pattern is also important in treatment for renal trauma, renal artery embolization, vascular reconstruction surgeries in treatment of congenital lesions and in surgery for abdominal aortic aneurysm. In the present case since the main right renal artery is also giving origin to inferior phrenic artery (which in turn gave origin to superior suprarenal artery) and inferior suprarenal artery with the absence of middle suprarenal artery, special care must be taken during renal surgeries as ligation of this renal artery will cut off blood supply not only to right kidney but also to the right suprarenal gland and part of right diaphragm. Hence such arterial variations must be detected by arteriography prior to surgery. In conclusion the authors believe that today renal transplants, interventional radiological procedures and urologic operations are done routinely. Awareness of the possible variations in the branching pattern of abdominal aorta in relation to arterial supply to the kidney is necessary for correct surgical management in such maneuvers.
CONCLUSION
The present article reports quadrifurcation of the main right renal artery into inferior phrenic artery, inferior suprarenal artery and 2 duplicate renal arteries. Though individual variations of each of these arteries have been reported, occurrence of variation in all these arteries in one single individual is a rare hitherto unreported observation. Transplanting a kidney with renal arterial variation involves higher morbidity but because of increasing demand for kidney transplantation, transplanting kidneys with multiple arteries by microvascular surgery has become necessary. In these circumstances in order to know the vascular pattern and to plan the surgery, it is essential to investigate patients by computerized tomography and arteriography prior to surgery.
ACKNOWLEDGEMENT
The Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to the authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of funding: As this study was carried out in the dissection hall of our Department, there was no separate financial aid provided for it. Conflict of interest: There is no conflict of interest Contribution details: • Concept, Design, Definition of intellectual content: Dr V K Bharambe, Dr Amol Shinde • Literature search: Dr V K Bharambe, Dr Amol Shinde • Clinical studies, Data acquisition, Data analysis: Dr VK Bharambe, Dr Amol Shinde • Manuscript preparation, Manuscript editing, Manuscript review: Dr VK Bharambe, Dr Amol Shinde
References:
1. Budhiraja Virendra, Rastogi Rakhi,Asthana Ak. Renal artery variations: embryological basis and surgical correlation.Rromanian Journal of Morphology and Embryology 2010; 51(3):533–536.
2. Kanaskar N, Paranjape V, Kulkarni J, Shevade S. Double Accessory Right Renal Arteries. IOSR Journal of Dental and Medical Sciences 2012;1(5):17-20.
3. Bergman RA, Cassell MD, Sahinoglu K, Heidger PM. Human doubled renal and testicular arteries. Ann Anat 1992;174(4):313-315.
4. Topaz O, Topaz A, Polkampally PR, Damiano T, King CA. Origin of a common trunk for the inferior phrenic arteries from the right renal artery: a new anatomic vascular variant with Clinical implications. Cardiovascular Revascularization Medicine 2010;57–62.
5. Moore KL, Dallay AF,Agur AM(Eds). Clinically oriented Anatomy, Wolters Cluwer, Lippincott Williams and Wilkins Publishers, New Delhi,2006;294-301.
6. Standring Susan, Ellis H, Healey JC (Eds), Gray’s anatomy: the anatomical basis of clinical practice, Elsevier–Churchill Livingstone Publishers, London, 2005 1274–1275.
7. Rao RT, Rachana. Aberrant renal arteries and its clinical significance:a case report.IJAV 2011;4:37-39.
8. Shinde A, Rao MP, Mishra PP, Paranjape V. Tortuous abdominal aorta with right testicular vein terminating into right renal vein. A report from cadaveric dissection. Med J D Y Patil Univ 2013;6:334-37.
9. Shinde A, Bharambe V. A Cadaveric study of lower polar supernumerary renal arteries-Embryological and clinical consideration. IOSR Journal of Dental and Medical Sciences 2014;13(7):06-09.
10. Mehta G, Arole V. Accessory renal arteries: A cadaveric study. International Journal of Biomedical and advanced Research 2014;05(04).
11. Patel S, Wanjari A, Naik A, Deshpande J. A case Report:double renal arteries. IJAV 2012;5:22-24.
12. Budhiraja V, Rastogi R, Bankwar V, Sathpati DK. Hilar renal arteries: A morphological study from central India with clinical correlation. Eur J Anat 2012;16(3):167-171.
13. Panagouli E, Lolis E, Venieratos D. Bilateral origin of the testicular arteries from the lower polar accessory renal arteries. Int J. Morphol 2012;30(4):1316-1320.
14. Felix W. Mesonephric arteries (aa. mesonephricae). In: Kiebel F, Mall FP eds. Manual of human embryology Vol 2. Philadelphia, Lippincott. 1912; 820–825.
15. Brannen GE, Bush WH, Correa RJ Jr, Gibbons RP, Cumes DM. Microvascular management of multiple renal arteries in transplantation. J Urol. 1982 Jul;128(1):112-5.
16. Kadotani Y, Okamoto M, Akioka K, Ushigome H, Ogino S, Nobori S, Higuchi A, Wakabayashi Y, Kaihara S, Yoshimura N. Management and outcome of living kidney grafts with multiple arteries. Surg Today 2005; 35: 459–466.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





