IJCRR - 7(4), February, 2015
Pages: 08-13
Print Article
Download XML Download PDF
Awareness regarding child care and sanitation: A generation dependent comparison among mothers of Purba
and Paschim Medinipur districts, West Bengal
Author: Madhumita Guria, Kausik Chatterjee, Sabyasachi Ray, Debidas Ghosh
Category: Healthcare
Abstract:Objectives: The study focuses the awareness level of mothers of previous and present generations about child care and sanitation in families of remote villages of Purba Medinipur and Paschim Medinipur with low socio-economic condition. Methods and materials: The study was completed by pre-tested structured questionnaire method. In this study 1330 mothers were randomly selected out of which 430 mothers from previous generation and 900 mothers from present generation were included. The remote villages of Purba and Paschim Medinipur districts of West Bengal were selected as study areas. Results: The result shows that there are not so much awareness about child care and sanitation in these remote villages. Mothers of present generation are found with more awareness than mothers of previous generation in all respect. Educational level, cast and occupational variation as well as exposure to the mass media plays a vital role for awareness generation about child care and sanitation among mothers. Conclusion: Government authority should take proper steps for the improvement of child care and sanitation through campaigning among family members as children are the backbone of the nation.
Keywords: Sanitation, Low socio-economic groups, Hygiene, Educational level, Mass media
Full Text:
INTRODUCTION
Health care is one of the important interventions in the process of economic and social development and improved their quality of life in different socio-economic families1 . The successful sanitation program in West Bengal first started in 1991 is now serving as a global model for developing countries2 . Water and sanitation related diseases became one of the most significant child health problems worldwide3 . In some cases these diseases cause premature death, but more frequently resulted in fatal chronic conditions such as diarrhea, worm infections, cholera, malaria, trachoma and schistosomiasis4 . Children who suffer constantly from water borne diseases are in disadvantages in school as poor health directly reduces cognitive potential and indirectly undermines schooling through absentees, attention deficits and early drop out 5 . With support from NGO’s (Non-Government Organization), UNICEF and local Government these programs play a major role in empowering workers. Midnapore has inspired the other districts of the state with 100% coverage where the overall sanitation coverage in West Bengal state is 65% and the national coverage of 32% 6 . Holistic development of needy children is projected to be achieved through empowerment of the community. There are some programmes initiated namely Aakar, Parivertan, Lakshya, Aahar Apurti, Uphaar for child care and development with a motto to make a bridge between the gap of under privileged street children and their counterparts 7 .
With the growing inflation in the pricing policies of companies, common people are forced to cut short their comers and limit the area of designs. However, when it comes to the safety and betterment of child, no parents would like to sacrifice with the quality8 . For working parents it becomes necessary to join some child care programme, working parents can adopt different ways from which they can gain benefits for child care health and development 9 . It is essential to find desiring child care assistance which selecting child care programme for the baby10. Education and communication are important components of a hygiene promotion programme. All people have a right to know about the relationship between water, sanitation, hygiene and the health of themselves and their families 11.
METHODOLOGY
The survey covered ten remote villages where five (5) villages (Mayna, Shilaberia, Bararankua, Gonara Gangadharbar) from Purba Medinipur district and 5 villages (Binpur, Pingla, Mandar, Kulasini, Chhatra) from Paschim Medinipur district under taken from June, 2007 to December, 2009. From these villages 430 mothers of previous generation (age group >20 to ≤ 55 yrs) and 900 mothers of present generation (age group >55 to ≤ 75 yrs) were randomly selected to include a total of 1330 mothers out of 150 families. They were dependent principally on agriculture and the rests were engaged with daily basis labour, private company and other type of jobs with average monthly income of Rs. 4000 to 5000 per month. Maximum couples had more than two children. This study framed with five questionnaire domains and each domain contains 10 marks. So, this was a total of 50 point of questions about child sanitation and hygiene. These domains were on
(i) Food Sanitation and Kitchen Sanitation- Cleaning of utensils before and after cooking; Washing hands at the time of cooking; Covering and preservation of storage food, Washing of hands of the elder family members at the time of serving; Serving of warm or cold food items.
(ii) Personal hygiene – Using of separate water container for washing, bathroom, latrine, kitchen; Washing of hands of mother or family members after blowing their noses, diapering of children; Hand washing of children during toileting; Use of sandals at the time of going to toilet or latrine.
(iii)Hygiene of Latrine/Toilet/Waste matter – Hygienic status of Latrine; Availability of water facility near the latrine or toilet; Using of hand-wash or soap after using latrine or toilet; Disposal of waste matters (vegetable skins after pilling, used diaper, excretory products of domestic pet animals) with a safe distance or not from the house.
(iv)Child and infant sanitation- Cleaning and washing of body parts after diapering of children; Regularity of bathing with proper cleaning with bathing soap, using any soap, detergent or sanitizer for cleaning their clothes.
(v) Bed room hygiene- Proper dustering of bed; Washing of bed cover or pillow cover, mosquito net with detergent and warm water; Cleaning and moping of floor of bed room on daily basis. These results were transferred into percentage and grade as per following gradation system

RESULTS
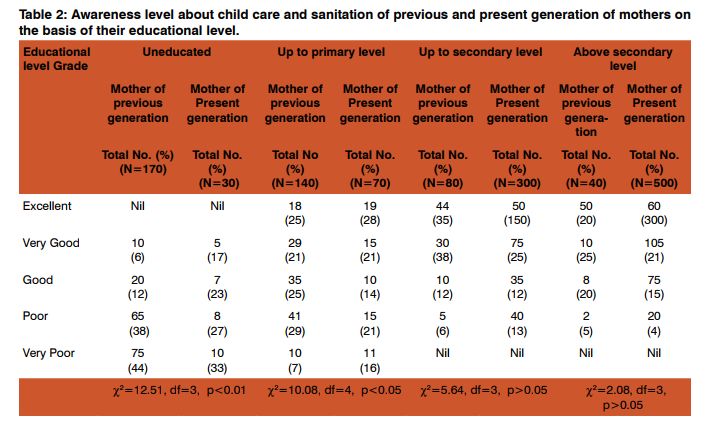
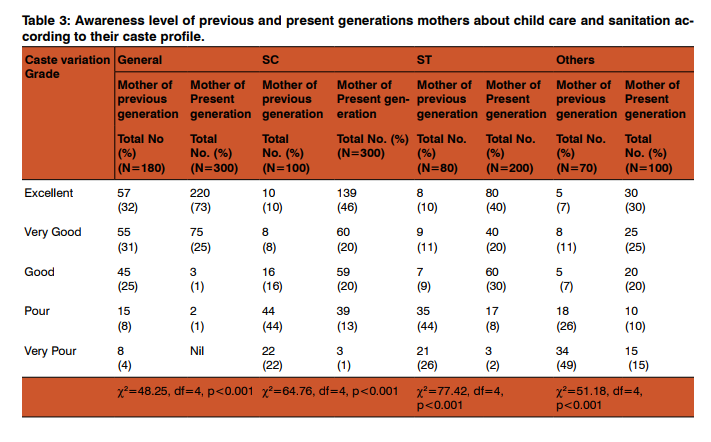
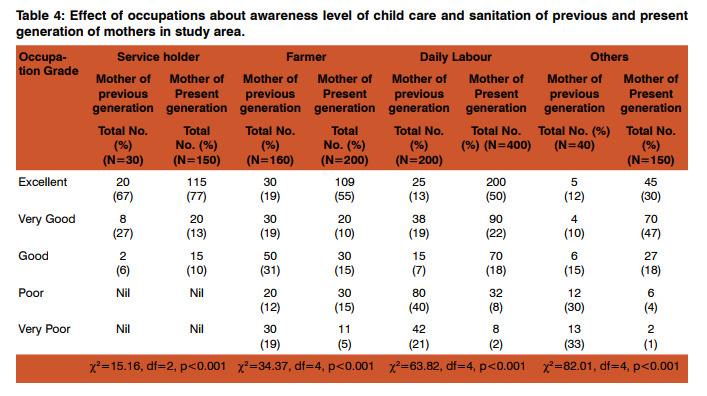
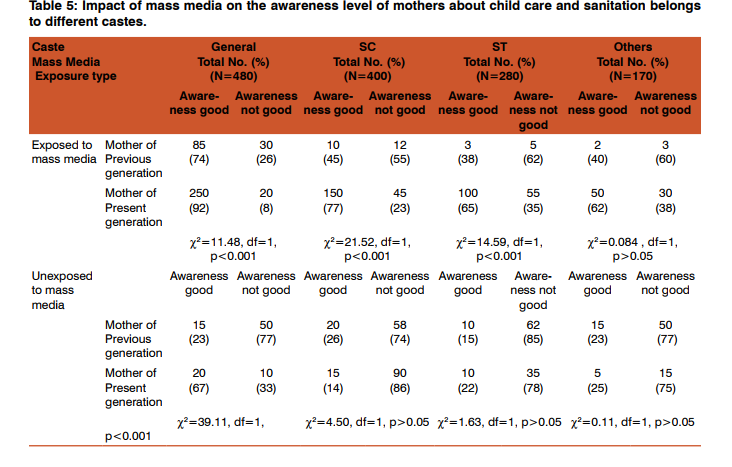
From two tail Chi-square test of independence, it was found that there was a significant (P0.05). These were strengthened here from the data expressed in percentage where in previous generation and present generation of mothers the awareness level becomes increased due to advancement of their educational level. In uneducated group, awareness level in maximum cases was ‘very poor grade’ in mothers of both the generations. But in above secondary group, awareness level in maximum cases was in excellent grade in present generation of mother (Table 2). From Chi-square test of independence, it was noted that there was a significant association between awareness level of child care and sanitation of previous and present generation of mothers with their caste profile. This result indicated here by the comparative analysis in percentage which focused that in general caste of both generation of mothers there maximum awareness was in excellent grade. In SC, ST and other caste, maximum grade of their awareness was in excellent in present generations, whereas in previous generations of mothers, these were in poor and very poor (Table 3). Analysis of collected data using two tail Chi-square test of independence, it was found that there was a significant (P<0.001) association between awareness level of child care and sanitation of mothers with their occupations. This result was in same line with the data expressed in percentage. In case of service holder group of both previous and present generations, excellent grade was more and there was no poor and very poor grade. But in farmer and daily labour and others groups of previous generation of mothers, the maximum percentage were in good and poor whereas in present generation of mothers it was excellent and very good grade (Table 4). Comparative analysis of awareness level of mothers about child care and sanitation belong to different castes of previous and present generations with mass media exposed and non exposed group, a significant (P<0.001) association was noted between caste variation with Mass Media exposure of or not of both the generation of mothers from Chi-square test of independence. This result was strengthen here by the comparative analysis of the result in percentage which focused that in Mass Media exposed group, in all caste of two generations, awareness level was more than the un-exposed to Mass Media group (Table 5).
DISCUSSION
Sanitation addressees the physical and operational environment as it applies to environmental health and safety 12. A child performs very actively, when his or her physical and mental health is good which depends on their hygienic life style 13. Hygienic lifestyle is maximally depends on their mother because the child spend their maximum time of the day with their mother. So, if mother’s life style is unhygienic then the child suffers from different types of diseases 14. From this study it was noted that awareness level of maximum mothers are poor. According to their educational level it was noted that maximum awareness was found in both generation of mothers belongs to secondary and higher secondary level than primary level and uneducated. So, it is clear that education is a factor for the awareness of the mother. Similarly both generations of mothers belongs to general caste are more aware than mothers belongs to SC, ST and other caste. The level of awareness is much higher than the other occupation in both generations of mothers. Mass media i.e. radio, television etc. also plays a vital role for the generation of awareness of mothers which are consistence with the reports of others 15. From these results it may be stated that though there was strong state and district level legislative agenda has put for the sanitation programme high on the developmental issue 16, 17 but there was no such strong awareness in these families. This may be due to lack of education, cast variation, occupation variation and also as an effect of media. So, it may be suggested that the Government authority should take proper step for the improvement of child care and sanitation through campaigning taking the help of NGOs and other Research Agencies like University, Colleges, in this concern18,19. National Social Service (NSS) Scheme which is running in colleges and universities may take some initiative in the awareness generations for the child care especially in remote villages and in slam areas of town 20. As prevention is better than cure so mothers will have to take steps against unhygienic life style for betterment of everyday life of their children.
CONCLUSION
As child health is the indicator of the healthy society, So the health of the child should be maintained properly as they are the backbone of the society. It may be suggested that government authority should take proper steps for the improvement of child care and sanitation through campaigning taking the help of the NGOs and other research agencies like University, Colleges in this concern. National Social Service (NSS) Scheme which is running in colleges and universities may take some initiative in the awareness generation for child care especially in remote villages and slum areas in towns.
Acknowledgement
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
1. Hawe P, Shiell A, RileyT, Gold L. Methods for exploring implementation variation and local context within a cluster randomised community intervention trial. Journal of Epidemiology and Community Health. 2004; 58: 788-793.
2. UNCF (United Nations Children’s Fund).Towards Better Programming: A Sanitation Handbook. Water, Environment and Sanitation Technical Guidelines Series No-3. A Sanitation Handbook. UNICEF’s Water, Environment and Sanitation Section, Programme Division and USAID’s Environmental Health Project. Environmental Health Project, Contract No. HRN-5994-C-00-3036-00, Project No. 936- 5994:1-81. UN Plaza, New York, USA, 1997.
3. Das, K. Rural Drinking Water Supply in India: Issues and Strategies, 207-277. In: Sebastian Morris (ed.), India Infrastructure Report 2001: Issues in Regulation and Market Structure, Oxford University Press, New Delhi, 2001.
4. WHO (World Health Organization). Tools for assessing the operation and maintenance status of water supply and sanitation in developing countries. Document WHO/SDE/ WSH/00.3. Water Supply and Sanitation Collaborative Council and Operation/Maintenance Network, WHO, Geneva, 2000
. 5. UNDP. Human Development Report 2006-Beyond Scarcity: Power, Poverty, and the Global Water Crisis, 2006, Pp. 45.
6. Narayanan R, Norden HV, Gosling L, Patkar A. Equity and Inclusion in Sanitation and Hygiene in South Asia: A Regional Synthesis Paper. UNICEF, Water Aid, Water Supply and Sanitation Collaborative Council Report, 2011, Pp.1- 17.
7. French G. Children’s early learning and development: A research paper. National Council for Curriculum and Assessment (NCCA), 2007, Pp.4-30.
8. AECDHB (Arizona Early Childhood Development and Health Board). High-quality child care and early education: what arizona’s parents want (First Things First). N Central Ave, Phoenix, AZ, 2012, Pp:1-88.
9. RIC. Getting the right start: National Service Framework for Children Standard for Hospital Services. Department of Health, RIC, United Kingdome, 2003, Pp.1-50.
10. Crosson-Tower C. The role of educators in preventing and responding to child abuse and neglect. Child abuse and neglect user manual series. U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, Office on Child Abuse and Neglect, 2003, Pp.1-79.
11. Child Action Inc. High quality child care, your guide to finding and selecting the best care for our child. Sacramento, CA, USA, 2013, Pp.31-42.
12. Cairncross S. Health Impacts in Developing Countries: New Evidence and New Prospects. Journal of the Institution of Water and Environmental Management. 1990; 4:571-577.
13. Ezzati M. Complexity and Rigour in Assessing the Health Dimensions of Sectoral Policies and Programmes. Bulletin of the World Health Organization. 2003; 81:458-459.
14. RCP (Royal College of Psychiatrists). London Physical health in mental health; Final report of a scoping group. Occasional Paper OP67, 2009, Pp.5-68.
15. Baran S, Chase L, Courtright J. Television drama as a facilitator of positive social behavior. The Waltons. Journal of Broadcasting. 1979; 23: 277-284.
16. Pendley C. A Demand-based Approach to Rural Water Supply and Sanitation. In: K. Pushpangadan (ed.), National Seminar on Rural Water Supply and Sanitation, Centre for Development Studies, Trivandrum, 1997.
17. Ponthiere G. Mortality, Family and Lifestyles. Journal of Family and Economic Issues. 2011; 32:175-190.
18. Andrews AB, McLeese DG, Curran S. The impact of a media campaign on public action to help maltreated children in Addictive families. Child Abuse and Neglect. 1995; 19: 921-932.
19. Maiti S, Ali KM, Dash SS, Ghosh D. Impact of ‘Child-toFamily’ Strategy for Health Awareness Improvement at Rural Sectors of Paschim Medinipur District, West Bengal. Online Journal of Health and Allied Sciences. 2010, 9: l-3.
20. Guria M, De D, Bera TK, Ghosh D. Awareness Level of Family Planning Practices in School Going Adolescent Girls of Different Socio-economic Groups in Rural Sectors, West Bengal. Journal of Human Ecology. 2009; 27:101-104.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





