IJCRR - 7(19), October, 2015
Pages: 26-30
Date of Publication: 10-Oct-2015
Print Article
Download XML Download PDF
EFFECT OF ULTRASOUND ON PAIN IN AMATEUR SQUASH PLAYERS WITH PATELLOFEMORAL PAIN SYNDROME
Author: Anil T. John, H.R. Rai, Vinod Kumar, Jimshad T.U.
Category: Healthcare
Abstract:Objectives of the study was to find out the effectiveness of Ultrasound therapy on pain in amateur squash players with patellofemoral pain syndromes. Total of 15 subjects (11 males and 4 females) were included in the study. All of the subjects were amateur squash players were diagnosed with chondromalacia patella by an Orthopedecian and referred for physiotherapy. Subjects who fulfilled the inclusion and exclusion criteria were selected by convenience sampling,. Informed consent was taken from each of the subjects prior to participation. Instructions were given to the subjects about techniques performed. A total of 15, subjects received UST exercises. Study concluded that UST along with exercises caused significant relief of pain and improvement in functional activity in amateur squash players with patellofemoral pain syndromes
Keywords: PFPS, US, Squash players
Full Text:
INTRODUCTION
Patellofemoral pain syndrome (PFPS) is very common in active individuals. Sports medicine centers report that there is 25% to 40% PFPS in sporting population.1 The common characteristic Patellofemoral pain syndrome (PFPS) is pain in front of the knee which is increased by activities like walking up and down stairs, sitting with flexed knees for long periods, running, kneeling and squatting2 (PFPS) affects both athletes and non-athletes. PFPS patients complain that pain is aggravated by daily activities. Patellar crepitation, swelling and locking are other symptom. Patellofemoral pain syndrome can be caused by direct trauma to the knee, or the cause can be insidious in nature., such as poor hip rotation control, excessive foot pronation, femoral anteversion, tibial torsion, bone configuration, or tight muscles are thought to cause PFPS because of altered lowerextremity biomechanics Vastusmedialis oblique muscle dysfunction also has been proposed as a contributor to altered patellofemoral kinematics. 4 A critical review of squash epidemiological studies indicated that squash players most commonly report acute soft-tissue injuries at hospital emergency departments. Lower-limb injuries account for the majority of the injuries sustained by squash players. The knee and ankle joint are reportedly the most commonly injured body regions in squash. Some of the factors that may increase your risk of injury include age, poor fitness level, poor technique – puts unnecessary strain on joints and muscles.[18] Squash requires high-speed movements around the court while maintaining control over ball placement and is a high intensity sport. The players need large range of joint motion and velocity of limb action in order to hit the ball. the physical demands of the sport, the speed, size and physical properties of the ball, court surfaces, the confined area of play and close proximity of players while swinging a racket causes the risk of injury which is about 45%. [20] In this sport, 58% of injuries affected the lower limb. Injuries in squash players most frequently affected the knee, lumbar region, ankle and muscles, especially the calf. In comparison with the tennis (21%) and badminton (21%) Squash players face up more injuries (59%). On the other hand, injuries to the lower limbs in squash are common and relate to the acute physical stresses increase in the nature of the sport, as well as the more chronic overuse type of injuries. Since players are active for most time of the game, they may face more sport injuries.
[21]A study showed that knee injuries seen in squash players are collateral ligament (33%), patello femoral (23%), patella dislocation, meniscal (19%), cruciate ligament (6.8%) traumatic synovitis (9%) other (6.7%).[19] The American Physical Therapy Association’s Guide for Physical Therapist Practice recommends the use of therapeutic modalities for a variety of musculoskeletal conditions, including PFPS. A combination of physical therapy and NSAIDs (non-steroidal anti-inflammatory drugs) is also very effective in reducing pain for patients who are suffering from PFPS. Therapeutic ultrasound is one of many rehabilitation interventions available for reducing pain and inflammation. “Ultrasound is a form of mechanical energy consisting of high frequency vibrations”. These vibrations result in acoustic streaming and radiation forces, which enhance the flow of particles from one side of a cell membrane to the other. Thus, ultrasound increases cell permeability. Pulsed ultrasound is generally recommended for treatment of pain and inflammation in acute stages, while the continuous ultrasound is recommended for reducing the swelling. It has also been observed that patients who have been diagnosed with PFPS and who have neglected therapy have developed osteoarthritis of the knee joint. There has been a variety of treatments prescribed for relief pain in patients with PFPS but has been found to have recurred because of lack of fitness, so the aim of this study is to find out whether ultrasound has any effect in the reduction of pain of PFPS in amateur squash players.
Objectives of the study:-was to find out the effectiveness of Ultrasound therapy on pain in patellofemoral pain syndromes in amateur squash players.
Null hypothesis (Ho ): Ultrasound therapy will have no effect on pain in amateur squash players with patellofemoral pain syndrome
Experimental hypothesis (H1 ) Ultrasound therapy will have significant effect on pain in amateur squash players with patellofemoral pain syndrome,
METHODS
Total of 15 subjects (11 males and 04 females) were included in the study. All of the subjects were amateur squash players were diagnosed as chondromalacia patella by an Orthopedecian and referred for physiotherapy. All of the Subjects diagnosed with chondromalacia patellae who fulfilled the inclusion criteria were included. Subjects between the age group of 18 – 45 years, both males and females were included. And subjects who had exclusion criteria of any fractures in and around the hip, knee and ankle, Subjects diagnosed with osteoarthritis of knee, Subjects above 45 years of age, Subjects with any systemic diseases were excluded. An experimental pre- post study designed, all the patients were recruited from Squash center at Jayanagar 5th block, Bangalore. Total duration of the study was 8 months and pre post measurement of outcome assessed for statistical analysis. Subjects who fulfilled the inclusion and exclusion criteria were selected by convenience sampling,. Informed consent was taken from each of the subjects prior to participation. Instructions were given to the subjects about techniques performed. A total of 30, subjects received UST and exercises
Ultrasound Therapy: The subject underwent ultrasound therapy with an intensity of 1W/cm2 for 8 minutes using a pulsed mode 1: 1 ratio with frequency of 1MHz for 3 sessions per week was given for 4 weeks
Strengthening exercise
DAPRE REGIMEN: The Daily Adjustable Progressive Resistance Exercise(DAPRE) technique is more systematic and takes into account the different rates at which individuals progress during rehabilitation and conditioning programs. The system is based on a 6RM working weight. The adjusted working weight, which is based on maximum number of repetitions possible using the working weight in a set #3 of the regimen, determines the working weight of the exercise session.
Data Analysis
• Data analysis was performed by SPSS (version 17) for windows. The alpha value is set as 0.05.
• Descriptive statistics was used to find out mean, standard deviation and range for demographic and outcome variable.
• Wilcoxen signed Rank test will be used to find out the significant difference for ordinal scales within the group
• Paired t-test will be used to find out homogeneity for baseline and demographic and ratio outcome variable within the group.
• Chi square test was used to find out gender differences among the two groups. • Microsoft word, excel was used to generate graph and tables etc.
RESULTS
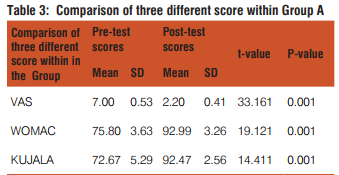
In the Group pre VAS mean is 7.00 with standard deviation of 0.53 and post VAS is 2.20 with standard deviation of 0.41 which was statistically significant to the p-value 0.001. Pre WOMAC score is 75.80 with standard deviation of 3.63 and Post WOMAC is 92.99 with standard deviation of 3.26 which was statistically significant with p-value 0.001 . Pre KUJALA is 72.67 with standard deviation of 5.29 and Post.
KUJALA is 92.47 with standard deviation of 2.56 which was statistically significant to the p-value 0.001.
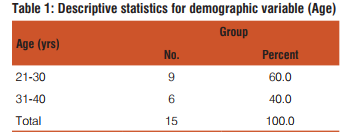
Table 1 Data are number and percent of age. Mean percent of the Group between the age of 21 – 30 is 60 % and mean percent of Group between the age of 31 – 40 is 40 % . The number of subject within the age group of 21-30 is 9 and the number of subject within the age group of 31-40 is 6.
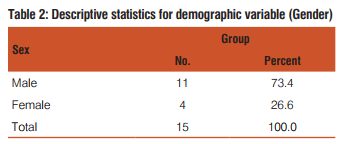
Table 2 Data are number and mean percent of gender. Mean percent of Males is 73.4 %. Number of male subjects is 11 and Mean percent of Females is 26.6, Number of female subjects is 4.
DISCUSSION
The purpose of the study was to find out the effectiveness of Ultrasound therapy on pain in amateur squash players with patellofemoral pain syndromes. Baseline data of demographic and outcome Variable did not show any significant difference in patient population. All the patients were able to finish the study. For the Group the Pre VAS Score was 7.00 and the Post test score was 2.20 following treatment and was statistically significant with p value 0.001. Also, the pre KPSS Score was 72.67 and the Post test score was 92.47 and was statistically significant with p value 0.001. Then, the Group Pre WOMAC was75.80 and the Post test score was 92.99 and was statistically significant with p value 0.001. Group was given ultrasound and strengthening exercises. The outcome measures used were VAS, KPSS and WOMAC. There was tremendous decrease in pain, increase in the KPSS score and increase in the WOMAC score. Pain reduction also enhanced patient compliance with the rehabilitation programme, and improved patients satisfaction and was used as an inexpensive adjunct to a rehabilitation programme in the management of PFPS. This is supported by study done by Hartley Therapeutic ultrasound is one of many rehabilitation interventions available for reducing pain and inflammation. “Ultrasound is a form of mechanical energy consisting of high frequency vibrations” These vibrations result in acoustic streaming and radiation forces, both of which enhance the flow of particles from one side of a cell membrane to the other. Thus, ultrasound increases cell permeability. As a result of stable cavitations ultrasound also “exerts mechanical stresses on the surrounding cells or other structures” This statistical significance in outcome was due to the healing effect of ultra sound which helps in reduction of pain and inflammation, this was also compounded with the fact that exercises helped in reducing the frictional forces of patella on lower end of femur and upper end of tibia, thereby giving the part rest as well as sufficient time for healing to take place. Heintjes EM, Berger M stated that effectiveness of exercise therapy in reduces anterior knee pain and improves knee function in patients with PFPS. Quadriceps strength is strongly associated with knee pain and disability in the community, even when activation and psychological factors are taken into account. This has important therapeutic implications.
Limitations of the study
The sample being small and convenient limits the population to which the results can be confidently applied, the duration of the study and the recommended sessions were less which again limits study, Long term follow up was not done.
Recommendations for further study The future scope of the study include the studies with a larger sample size should be conducted, studies with longer duration are recommended, recommendation for longer follow up for long term benefits, studies with different treatment combined with our treatment approaches can be done, different duration of exercises and ultrasound dosages can be used and studied further in treatment of PFPS.
CONCLUSION
UST along with exercises caused significant relief of pain and improvement in functional activity in amateur squash players with patellofemoral pain syndromes.
ACKNOWLEDGEMENT
Authors acknowledge the immense helprecieved from the scholars whose articles are cited and included in references in the manuscript. The authors are also grateful to authors / editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. S.T. Green. Patellofemoral syndrome, Judah Street 2717, San Francisco, Journal of Bodywork and Movement Therapies (2005) 9, 16–26.
2. Gregory R Waryasz and Ann Y McDermott. Patellofemoral pain syndrome (PFPS): a systematic review of anatomy and potential risk factors. Dynamic Medicine 2008; 10.1186/1476-5918-7-9.
3. Konstantinos D. Papadopoulos, Jane Noyes, Moyra Barnes, Jeremy G. Jones, Jeanette M. Thom. How do physiotherapists assess and treat patellofemoral pain syndrome in North Wales? A mixed method study. International Journal of Therapy and Rehabilitation, May 2012, Vol 19, No5.
4. G.Y.F, A.Q. Zhang. Biofeedback exercise improved the EMG activity ratio of the medial and lateral vasti muscles in subjects with patellofemoral pain syndrome. G.Y.F. Ng et al. / Journal of Electromyography and Kinesiology 18 (2008) 128–133.
5. Erik Witvrouw, S. Werner, C. Mikkelsen, D. Van Tiggelen, L. Vanden Berghe, G. Cerulli. Clinical classification of patellofemoral pain syndrome: guidelines for non-operative treatment. Knee Surg Sports Traumatol Arthrosc (2005) 13: 122–130.
6. Heintjes EM, Berger M, Bierma-Zeinstra SMA, Bernsen RMD, Verhaar JAN, Koes BW. Exercise therapy for patellofemoral pain syndrome (Review).The Cochrane Collaboration and published in The Cochrane Library 2009, Issue 1.
7. Cristina Maria Nunes Cabral1, Angela Maria de Oliveira Melim, Isabel de Camargo Neves Sacco, Amelia Pasqual Marques. Effect of a closed kinetic chain exercise protocol on patellofemoral syndrome rehabilitation, OuroPreto – Brazil, ISBS Symposium 2007;688.
8. Carina D. Lowry, Management of Patients with Patellofemoral Pain Syndrome Using a Multimodal Approach: A Case Series. Journal of orthopaedic and sports physical therapy | volume 38 | number 11 | November 2008 | 691.
9. Christian J. Barton, Hilton B. Menz. Evaluation of the Scope and Quality of Systematic Reviews on Non-pharmacological Conservative Treatment for Patellofemoral Pain Syndrome. Journal of orthopaedic and sports physical therapy | volume 38 number 9 September 2008 | 529.
10. McConnell J. The management of chondromalacia patellae: a long term solution. Aust J Physiother. 1986;32:215–223.
11. Mark Overington, Damian Goddard, Wayne Hing. A critical appraisal and literature critique on the effect of patellar taping – is patellar taping effective in the treatment of patellofemoral pain syndrome?.New Zealand Journal of Physiotherapy 34(2): 66-80.
12. Sheehan FT, Derasari A, Brindle TJ, Alter KE. Understanding patellofemoral pain with maltracking in the presence of joint laxity: complete 3D in vivo patellofemoral and tibiofemoral kinematics. J Orthop Res. 2008;27:561–570.
13. Wilson NA, Press JM, Koh JL, et al. In vivo and noninvasive evaluation of abnormal patellar tracking during squatting in patellofemoral pain. J Bone Joint Surg Am. 2008;91:558–566.
14. Boucher JP, King MA, Lefebvre R, Pepin A. Quadriceps femoris muscle activity in patellofemoral pain syndrome. Am J Sports Med. 1992;20:527–532.
15. Cowan SM, Bennell KL, Hodges PW, et al. Delayed onset of electromyographic activity of vastusmedialisobliquus relative to vastuslateralis in subjects with patellofemoral pain syndrome. Arch Phys Med Rehabil. 2001;82:183–189.
16. Karst GM, Willett GM. Onset timing of electromyographic activity in the vastusmedialis oblique and vastuslateralis muscles in subjects with and without patellofemoral pain syndrome. Phys Ther. 1995;75:813–823.
17 Powers CM. Patellar kinematics, part I: the influence of vastus muscle activity in subjects with and without patellofemoral pain. PhysTher. 2000;80:956–964.
18. L Meyer, L van Niekerk, E Prinsloo, M Steenkamp, Q Louw. Prevalence of musculoskeletal injuries among adolescent squash players in the Western Cape. SAJSM vol 19 No. 1 2007.
19. M. D. Chard and S. M. Lachmann. Racquet sports patterns of injury presenting to a sports injury cunic. Brit.J. Sports Med1987, December Vol. 21, No. 4, pp. 150-153.
20. David A. Lake, Nancy H. Wofford. Effect of Therapeutic Modalities on Patients With Patellofemoral Pain Syndrome. Sports Health: A Multidisciplinary Approach March/April 2011vol. 3 no. 2 182-189.
21. Brosseau L, Casimiro L, Welch V, Milne S, Shea B, Judd M, Wells GA, Tugwell P. Therapeutic ultrasound for treating patellofemoral pain syndrome (Review). The Cochrane Library 2009, Issue 1.
22. Ann-Katrin Stensdotter, Paul W. Hodges, Rebecca Mellor, Gunnevi Sundelin, And Charlotte Ger-Ross, quadriceps. Activation in Closed and in Open Kinetic Chain Exercise. Submitted for publication December 2002.
23. Carolyn Kisner, Lymn Allen Colby. Therapeutic Exercise Foundations and Techniques. 5th edition:p-207.
24. H. Minoonejad , R. Rajabi , E. Ebrahimi-Takamjani, M.H. Alizadeh, A.A. Jamshidi , A. Azhari and E. Fatehi . Combined open and closed kinetic chain exercises for patello femoral pain syndrome , randomized controlled trial.World Journal of Sport Sciences 6 (3): 278-285, 2012.
25. Bert M. Chesworth, E Lsie G. Culham, G. Elizabeth Tata, M Alcolm Peat. Validation of Outcome Measures in Patients with Patellofemoral Syndrome, 302 chesworth et al jospt, February 1989.
26. K. Steininger and R. E. Wodick. sports-specific fitness testing in squash. Brit J. Sports Med. - Vol. 21, No. 2 June 1987, pp. 23- 26.
27. Burton L. Berson. An Epidemiologic Study Of Squash Injuries. The American Journal of Sports Medicine. March 1981 vol. 9 no. 2 103-106.
28. Anil Bhav, Erin Baker, Prescribing Quality Patellofemoral Rehabilitation before Advocating Operative Care. Rubin Institute for Advanced Orthopedics 2008.
29. Guilherme Lotierso Fehr1, Alberto Cliquet Junior, Enio Walker Azevedo Cacho3 and João Batista de Miranda. Effectiveness of the open and closed kinetic chain exercises in the treatment of the patellofemoral pain syndrome. Rev Bras Med Esporte Mar/ Abr, 2006. Vol. 12, No: 2; 3911-1345.
30. Daniëlle A.W.M. van der Windt, Geert J.M.G. van der Heijden, Suzanne G.M. van den Berg, Gerbenter Riet, Andrea F. de Winter, Lex M. Bouter. Ultrasound therapy for musculoskeletal disorders: a systematic review.7 January 1999; accepted 11 January 1999.
31. Anthony Keeley, Paul Bloomfield, Peter Cairns and Robert Molnar. Iliotibial band release as an adjunct to the surgical manage-ment of patellar stress fracture in the athlete: a case report and review of the literature. Sports Medicine Arthroscopy, Rehabilitation, Therapy and Technology 2009. 30 July
32. Roos EM, Klässbo M, Lohmander LSScand J Rheumatol. WOMAC osteoarthritis index. Reliability, validity, and responsiveness in patients with arthroscopically assessed osteoarthritis. Western Ontario and MacMaster Universities.1999; 28:210-5.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





