IJCRR - 10(15), August, 2018
Pages: 01-05
Date of Publication: 16-Aug-2018
Print Article
Download XML Download PDF
Platelet Rich Fibrin & Guided Tissue Regeneration Aided Coverage of a Mucosal Fenestration \? An Interdisciplinary Approach
Author: Divya S., Deepika P. C., Ambikathanaya
Category: Healthcare
Abstract:Aim: Mucosal fenestrations affecting permanent teeth are clinically challenging because they require a more complex approach. The objective of this case report was to describe a treatment modality used to manage an apical fenestration placed on the left mandibular central incisor root. Case Report: The case report describes the management of a patient with mucosal fenestration of root apex. Mucosal fenestration of root apex was treated by a combination of root canal treatment and surgery. Root-end resection was performed to bring the root apex within the alveolus before root-end filling and packing of the bony defects with platelet rich fibrin. The dehiscence of the buccal labial plate was managed by placement of a barrier membrane. The edges of the soft tissue defect was then deepithelialized, approximated and sutured. Discussion: Various treatment modalities advocated in the literature for the management of mucosal fenestration include- root canal treatment and root-end resection, blind root surface instrumentation and mouth rinsing with chlorhexidine, full thickness mucogingival flap with primary or secondary healing, pedicle flap operations, epithelialized and non-epithelialized grafting procedures for root coverage and full thickness mucogingival flaps with guided tissue regeneration and bone grafting. Conclusion: The endodontic and periodontal surgical techniques used in the management of alveolar or mucosal fenestrations alone are unremarkable but combining them can give optimum outcome.
Keywords: Platelet rich fibrin, Mucosal fenestration, GT
Full Text:
INTRODUCTION:
The relationship between the alveolar bone and the teeth have been dated back to 1963, when O’Connor studied the relationship of teeth with the tooth anatomy, inter-proximal bone, bony wedges and the presence of fenestrations.1 Fenestrations and dehiscences, are being more considered normal variations with regard to presence of the teeth, than pathologic conditions. The criteria for their identification as put forth by Davies RM et al 2. as dehiscence is a lack of cortical bone at the level of the root of the tooth, at least 4 mm apical to the margin of the inter-proximal bone; whereas fenestration is a contained defect of the alveolar bone that exposes the apical or the middle third of the root surface, without involving the marginal bone.
A precise and seldom encountered spectacle is a combination of apical fenestration along with a mucosal fenestration. Mucosal or apical fenestration is termed as a pathologic condition which is characterized by the perforation of the cortical plate and the overlying mucosa by the prominent roots of teeth. It was first described in literature as ‘‘bone fenestration by roots of deciduous teeth’’ by Mene´ndezin 19673. Mucosal fenestration may be attributed to decreased thickness of the alveolar housing, labioversion of the tooth in the dental arch, contour of the root apex, occlusal factors, orthodontic tooth movement, periodontal and endodontic pathology and aberrant frenal attachment.4,5,6
Mucosal fenestration is most frequently found in the mandibular or maxillary anterior teeth region, particularly on the labial aspect because of tooth angulation that places the root apices in alabial version. Mucosal fenestrations have been reported in literature but are far less prevalent as compared to normal fenestration perhaps due to symptom free nature.7Even though they are usually symptom-free, they might act as plaque-retaining areas, resulting in irritation and inflammation of the surrounding mucosa.8
Mucosal fenestrations affecting permanent teeth are clinically challenging because they require a more complex approach. The aim of this case report was to represent a treatment modality used to manage an apical fenestration occured on root surface of the left mandibular central incisor.
CASE REPORT:
A 26 year old male patient reported to the OPD of JSS Dental College and Hospital, Mysore with discoloured lower front tooth. Patient gave a history of trauma 1 year back, following which there was a progressive discoloration of the tooth with intermittent pus discharge. Patient was in good health. No pathologic signs were evident through facial inspection. Oral examination revealed the apical third of the root of 31 that perforated the buccal cortical plate and adjacent alveolar mucosa, being therefore exposed to the oral environment and the discoloured crown of the same tooth. [Fig:1]

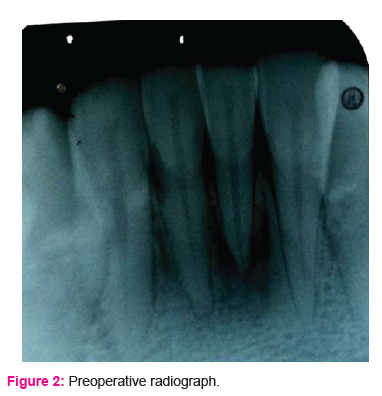
There was presence of plaque, calculus and soft debris on the exposed root tip and the margins of the surrounding mucosa were inflammed and tender. The tooth was grade 1 mobile. Pretreatment radiograph revealed discontinuity in the lamina dura around the apex of the 31 with periapical radioluscency [Fig:2]. Also, the tooth was nonvital. The probing depth measured 2mm buccally and 1.5 mm lingually hence, diagnosis of asymptomatic chronic apical periodontitis with mucosal fenenstration on tooth 31 was made.
TREATMENT:
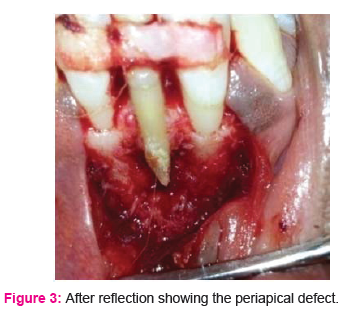
After phase 1 therapy consisting of scaling and root planing, multivisit endodontic treatment was performed. Following working length determination, biomechanical preparation was done using K-file and recapitulation with 5.25% sodium hypochlorite.calcim hydroxide paste was used as intracanal medicament for 10 days. Next appointment, calcium hydroxide paste was removed and root canal was obturated with cold lateral condensation of gutta percha with zinc oxide ugenol as sealant. Surgery was undertaken 2 weeks after endodontic treatment. Fibre reinforced composite splinting was done in relation to 41,31 and 32. Region 31,32,41,42 was anaesthetized with 2% lignocaine. Crevicular and vertical releasing incisions were made, and full-thickness flap was raised, revealing dehiscence of the buccal cortical bone along the root surface of 31 [Fig:3]
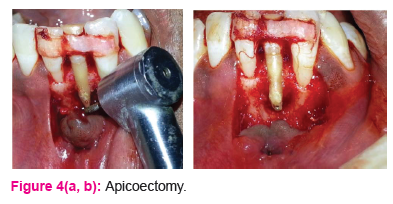
Granulation tissue was immediately apparent surrounding the root apex. Curettage of this tissue revealed the extent of bone loss. The prominent portion of the affected root apex was resected.
The resection was carried up to the level of remaining sound alveolar bone, so that the root margins were flush with the surrounding bone to reposition the affected root in the alveolar housing [Fig. 4a,b].
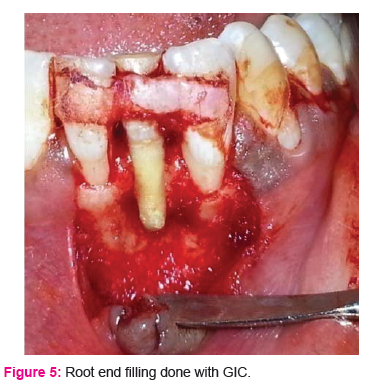
Any remaining granulation tissue was removed. The root planning was done and then glass ionomer cement(GC Fuji II; GC America, Alsip, IL)was placed over the prepared root end.[Fig: 6]
Autologous graft (platelet rich fibrin) was obtained from the patient and placed in the defect at the periapical region of 31. The root was then covered with GTR membrane (Healiguide).[Fig:6,7]

The edge of the mucosal defect was de-epithelialized, approximated and sutured with resorbable sutures to ensure closure [Fig:8]. The wound was covered with periodontal dressing (coe-pak)

Post-operative instructions were given and antibiotics and analgesics were prescribed.
Patient was recalled after 1 week for removal of the pack. Patient was without any local complications and free of symptoms. The 2 and 5 months recall showed excellent soft tissue healing [Fig:9a ,b]

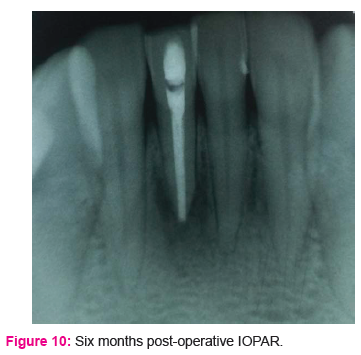
Periapical radiograph revealed well performed endodontic treatment, healing and remodelling of the apical area at 6 months recall [Fig:10]. A two year follow-up period with every 6 months radiographic evaluation was recommended.
DISCUSSION:
Mucosal fenestration is a relatively uncommon complication of pulpo-peri radicular disease.9,10,11 The exact aetiology is unknown but review of literature suggests that abnormally labioversed root tips, very thin labial plates and the presence of chronic periapical inflammation may be the probable cause. The first step toward management of mucosal fenestrations is identifying the precipitating cause of its occurrence. In this case, trauma could be the primary etiologic factor, along with prominent root positions and chronic periapical inflammation that might have destroyed the overlying thin facial cortex and mucosa. Mucosal breakdown and exposure of the root tip to the oral cavity leaves the root-tip vulnerable to plaque accumulation and calculus formation which prevents the reformation of mucosal covering.
Various treatment modalities advocated in the literature for the management of mucosal fenestration include- root canal treatment and root-end resection,8,9 blind root surface instrumentation and mouth rinsing with chlorhexidine10, full thickness mucogingival flap with primary11 or secondary healing12, pedicle flap operations4, epithelialized and non-epithelialized grafting procedures for root coverage and full thickness mucogingival flaps with guided tissue regeneration and bone grafting13.
In this case, since the tooth was non vital, it was first treated by root canal therapy to eliminate the focus of infection. Healing of the mucosa was then aided by removal of the granulation tissue, root end resection, and removal of adjacent infected cementum by root planning. The main objective of resection of the abnormally prominent root apices about the level of remaining sound alveolar bone is to return the root within the bony limit of the cortex. This affords a favourable anatomic configuration and eliminates future risk of irritation. Glass ionomer cement was used to achieve a good apical seal after proper isolation. Jhaveri et al14 have reported light cure GIC to be a successful root end filling material.
In the present case, after flap elevation dehiscence of the labial cortical plate was seen. Hence an attempt to regenerate the periodontal supporting tissues was made utilizing the principles of guided tissue regeneration. GTR was used in our case not only as a root coverage procedure, but also as a strategy of endodontic surgery where the ultimate goal was to regenerate the attachment apparatus.
Scientific evidence indicates that principles of GTR can be successfully applied in endodontic surgery to correct alveolar bone defects confined to periapical region. Animal histological studies showed that complete bone filling of periapical bone cavities occurred after endodontic surgery only when a barrier for guided tissue regeneration was used, whereas extensive connective tissue filling of the defects was found after conventional endodontic surgery.
The present case is unique in that it is the first case to utilize platelet rich fibrin (PRF) as a grafting material. The three crucial factors for healing and soft tissue maturation are angiogenesis, growth factors and mesenchymal stem cell activity. PRF consists of a fibrin 3D mesh polymerized in a specific structure, incorporating platelets, leucocytes, growth factors and circulating stem cells.17 The concentrations of growth factors within the platelet concentrate up regulate cellular activity and subsequently promote periodontal regeneration in vivo. Fibrin, fibronectin, platelet derived growth factor (PDGF), vascular endothelial growth factor (VEGF) and transforming growth factor beta (TGF-β) in PRF aid in angiogenesis, tissue repair and regeneration.18 Hence owing to these advantages PRF was used as an effective biomaterial as projected in this case.
CONCLUSION:
The endodontic and periodontal surgical techniques used in the management of alveolar or mucosal fenestrations alone are unremarkable but combining them can give optimum outcome. Guided tissue regeneration in combination with platelet rich fibrin can successfully be used to treat fenestrated root apices.
Abbreviations:
GTR: guided tissue regeneration
GIC: glass ionomer cement
PRF: platelet rich fibrin
PDGF: platelet derived growth factor
VEGF: vascular endothelial growth factor
TGF-β: transforming growth factor beta
Acknowledgement :
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of interest: Nil
References:
-
O’Connor TW, Alveolar bony contours, A thesis submitted to the Faculty of Baylor University Dallas, Texas, 1963.
-
Davies RM, Downer MC, Hull PS, Lennon MA, Alveolar defects in human skulls, J Clin Periodontol, 1974, 1(2):107–111.
-
Mene´ndez OR. Bone fenestration by roots of deciduous teeth. Oral Surg Oral Med Oral Pathol 1967;24:654–8.
-
Ju YR, Tsai HY, Wu YJ. Surgical intervention of mucosal fenestration in a maxillary premolar: a case report. Quintessence Int. 2004;35:125e128.
-
Abdelmalek RG, Bissada NF. Incidence and prevalence of alveolar bone dehiscence and fenestration in dry human Egyptian jaws. J Periodontol 1973;44:586–8.
-
Edel A. Alveolar bone fenestrations and dehiscences in dry Bedouin jaws. J Clin Periodontol 1981;8:491–9.
-
Ling LJ. The treatment of fenestrated root: case reports. J Dent Sci. 1989;9:137e140
-
Dawes WL, Barnes IE. The surgical treatment of fenestrated buccal roots of an upper molar: a case report. Int Endod J 1983;16:82–6.
-
Lehman J III, Meister F Jr, Gerstein H. Use of a pedicle flap to correct an endodontic problem: a case report. Journal of Endodontics 1979;5, 317–20.
-
Lin LJ. The treatment of fenestrated root: case reports. Journal Dental Science1989; 9, 137–40.
-
Tseng C-C, Chen Y-HM, Huang C-C, Bowers GM Correction of a large periradicular lesion and mucosal defect using combined endodontic and periodontal therapy: a case report. International Journal of Periodontics and Restorative Dentistry 1995;15, 377–83.
-
Rawlinson A. Treatment of a labial fenestration of a lower incisor tooth apex. British Dental Journal1984; 156, 448–9.
-
Chen G, Fang CT, Tong C. The management of mucosal fenestration: a report of two cases. Int Endod J. 2009;42(2):156e164.
-
Jhaveri HM, Amberkar S, Galav L, Deshmukh VL, Aggarwal S, Management of mucosal fenestrations by interdisciplinary approach: a report of three cases, J Endod, 2010, 36(1):164–168.
-
Von Arx T, Cochran DL, Rationale for the application of the GTR principle using a barrier membrane in endodontic surgery: a proposal of classification and literature review, Int J Periodontics Restorative Dent, 2001, 21(2):127–139.
-
Pecora G, De Leonardis D, Ibrahim N, Bovi M, Cornelini R, The use of calcium sulphate in the surgical treatment of a ‘through and through’ peri radicular lesion, Int Endod J, 2001,34(3):189–197.
-
Choukron J, Diss A, Simonpieri A et al. Platelet rich fibrin. A second generation platelet concentrate. Part IV. Clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Rad Endod 2006; 101: e 56-e60.
-
Dvorak HF, Harvey VS, Estrella P, Brown LF, McDenagh J, Dvorak AF. Fibrin containing gels induce angiogenesis. Implications for tumor stroma generation and wound healing. Lab Invest 1987; 57: 673-86.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





