IJCRR - 4(15), August, 2012
Pages: 127-141
Date of Publication: 15-Aug-2012
Print Article
Download XML Download PDF
MALAYSIAN DIETARY GUIDELINES 2010 IN PRACTICE: ACCEPTABILITY AND APPLICABILITY OF NUTRITION DELIVERY TOOLS AMONG UNIVERSITY STUDENTS IN TERENGGANU, MALAYSIA
Author: Pei Lin Lua, Wan Putri Elena Wan Dali, Mohd Razif Shahril
Category: Healthcare
Abstract:Objective: To evaluate the acceptability and applicability of nutrition education delivery through three tools; 1) conventional lectures, 2) brochures and 3) text messages via short messaging system (SMS). Methods: A prospective, cross sectional study was conducted among university undergraduates in Terengganu, Malaysia. Included students firstly went through a 1-hour lecture followed by the provision of brochures and contents of text messages. They then completed an evaluation form. Data analysis was carried out using SPSS 16.0 utilising descriptive statistics. 116 undergraduates were enrolled (mean age=19.3). Results: Majority of male (91.9%) and female students (91.1%) rated the slides as comprehensible. Both genders (male=70.3%, female=74.7%) ranked the presentation as ?interesting? while, 64.7% of them ranked the information included as adequate. Brochures were considered to be at
least \"good\" with regard to its pictorial graphics (85.3%) and languages (81.9%). Most of the students were also generally contented with the information given through the SMS (86.2%). Overall, 94.0% of students believed that nutrition education delivery through a variety of methods can provide and enhance their awareness and knowledge. Conclusion: This provides early evidence that these tools are acceptable and applicable in assisting undergraduates improve their diet and undergo active lifestyle.
Keywords: Undergraduates, nutrition education, acceptability, applicability
Full Text:
INTRODUCTION
The most recent version of the Malaysian Dietary Guidelines (MDG) 2010 was launched on 25th March 2010 with the newly modified edition consisting of 14 key messages compared to the first version in 1999.1 A collection of 55 key recommendations established under these 14 key messages clearly indicate the government‘s efforts to ensure all Malaysians maintain a nutritious diet, healthy weight and adequate exercise in order to reduce the risk for chronic diseases in later life. Although the previous guideline was published 10 years ago, a study conducted by Norimah and comembers has unfortunately shown that about 63% of the respondents from 773 adults in Kuala Lumpur (aged between 18 to 59 years) were not aware of its existence.2 This finding might be one of the crucial factors leading to the increase in nutrition-related diseases such as cardiovascular disease, cancer, hypertension and diabetes.3-5 Hence, efforts to disseminate the information to all age group in Malaysia to enhance awareness of the latest MDG 2010 should be constantly initiated and maintained.
Numerous studies evaluating the incidence of unhealthy eating habits and sedentary lifestyle have demonstrated links to a high prevalence of overweight and obesity.6-7 These two factors were accepted as the major causes of morbidity and mortality.8 As such, health educators should promote education and intervention strategies that encourage improved dietary behaviors.6 One important pathway to dietary improvement is through delivering nutrition education. Nutrition education is defined as any set of learning experiences designed to facilitate voluntary adoption of eating and other nutrition-related behaviour conducive to health and well-being.9 It is recognised as an important component in programs and interventions related to health promotion and disease prevention. Nutrition education can be delivered in a variety of modes such as printed materials (booklets, brochures, leaflets and posters), lectures, via Short Messaging System (SMS) or web-based education.10-12 However, information or contents added in nutrition education tools must be evaluated before delivery to the target population.13 A review by Clayton indicated that there are seven criteria need to be focused in evaluating an education material.14 These criteria includes; 1) content, 2) literacy, 3) graphics, 4) layout and typography, 5) motivating principles, 6) cultural relevance and 7) feasibility. University students are the main targets for delivering nutrition education to improve their dietary habits, in order to reduce excess chronic disease burden and to produce healthy intellectuals in the future. This group is at a crucial stage in their life development as they encounter transition from parental control over lifestyle behaviors to assuming own responsibility for their health choices.15 This highlighted an opportunity to develop nutrition education delivery tools in order to disseminate the information from MDG 2010 in the form of conventional lecture, printed media (brochures) and SMS. In order to elucidate the acceptability and applicability of the nutrition education delivery tools, an evaluation instrument with constructive feedback is necessary so that it can be modified and used as an example of good practice.16 The evaluation is obtained through questionnaires targeting specific information which includes understanding, adequacy of information and visual appeal. As such, the goals of this study were to (i) develop nutrition education delivery tools and (ii) evaluate their acceptability and applicability of nutrition education delivery tools in a sample of university student population.
METHODOLOGY
Study design and sample selection
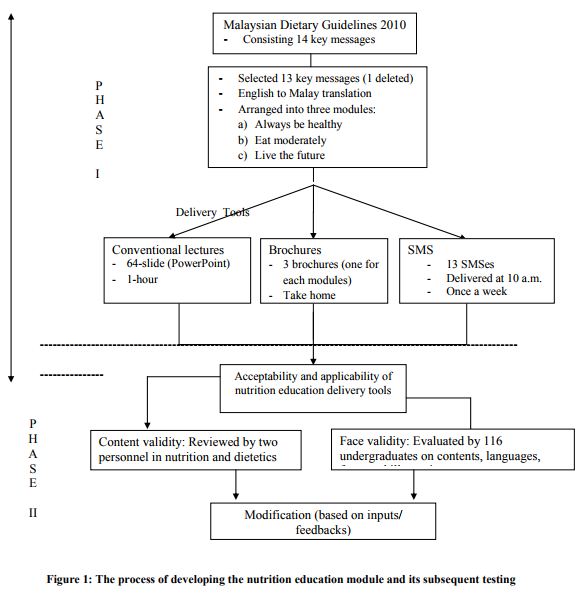
This investigation was based on a prospective, cross-sectional design which employed convenience sampling method. Participants were undergraduates who were studying in a local public university who met all the inclusion criteria. The inclusion criteria for the respondents were: (1) university students between the age of 18 to 20 years, (2) healthy, without any officiallydiagnosed diseases and (3) able to read, write, speak, and understand Malay or English. On the other hand, the exclusion criteria were: (1) respondents below or above the age range stated, (2) students in health science studies program, (3) students who declared chronic diseases diagnosis and (4) unable to read, speak or understand Malay or English. This study was carried out in twophase; 1) development of nutrition education delivery tools and 2) acceptability and applicability of nutrition education delivery tools.
Phase I – Development of nutrition education delivery tools
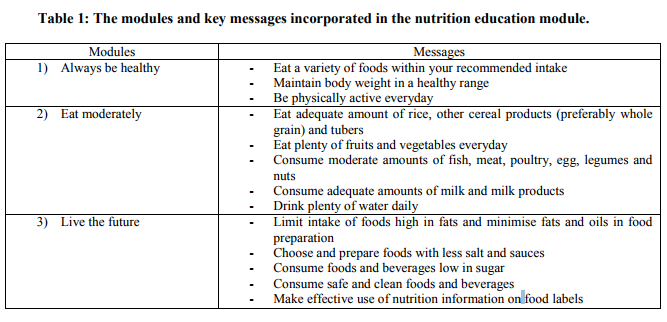
Phase I involved rearranging of the latest MDG 2010 to contain only 13 key messages (from the 14 original key messages). These messages were divided into three different modules; 1) Always be healthy (3 messages), 2) Eat moderately (5 messages) and 3) Live the future (5 messages)
(Table 1). Messages which deliberated on the Practise Exclusive Breastfeeding from Birth until Six Months and Continue to Breastfeed until Two Years of Age were excluded due to irrelevance to participants. All included messages were delivered through three modes; 1) conventional lectures, 2) brochures and 3) text messages via short messaging system (SMS). Conventional lectures were carried out in which all key messages in guidelines were compiled into a 64-slide multimedia Microsoft PowerPoint presentation. The slides used were clearly visible for approximately 100 students with appropriate font sizes. Attractive graphics and suitable combination colours were additionally used to stimulate their interest on the topics delivered in a 1-hour session. Brochures were designed to enhance their understanding and memory after the lecture, containing Key Recommendations and How to Achieve the recommendations for each message. Three brochures were developed, each representing the same three modules as presented in conventional lecture. The information was displayed on the coloured art papers in 35.8 cm x 25 cm-sized with four folded as well as doublesided printed. Pictorial graphics which includes food pictures, cartoon pictures and symbols were used to attract the readers. The text language was kept simple with black 12-font sized. Text messages via short messaging system (SMS) can be delivered through all forms of cellular telephone with a limitation of 152 characters for each 13 messages. All thirteen messages were designed to be delivered weekly and received at 10a.m. These text messages were manually delivered through the Mobile Nutritional Education System which was developed by Mobile Content and Services Provider based in Kuala Lumpur, Malaysia. SMSes and abbreviations were avoided to prevent misunderstanding of the information received. Although all information in conventional lecture, brochures and text messages were conveyed in Malay language, the original contents of the guideline were maintained and it had been reviewed by two qualified personnel in the field of nutrition and dietetics.
Phase II – Acceptability and applicability of nutrition education tools
Phase II aimed to evaluate the acceptability and applicability of all three nutrition education delivery tools developed in Phase I. Content validity was evaluated by two qualified researchers experienced in nutrition and dietetics while face validity was gauged by distributing Nutrition Education Tool’s Evaluation Questionnaire (NETEQ) to evaluate the students‘ understanding on the contents, presentation and illustrations showed in the slides, brochures and text messages. Subsequently, the tools were modified based on the inputs and feedbacks obtained from respondents recruited during this phase. Prior to data collection, an information sheet was given to all included participants to enhance their comprehension on the purpose of this study. Those who were willing to participate were requested to complete NETEQ for the purpose of evaluating the acceptability and applicability of these nutrition education delivery tools. A 1-hour lecture and brochures were delivered in original setting while all the intended 13 messages text messages were only shown on a piece of laminated paper (Appendix 1). To ensure the performance and functionality of the Mobile Nutritional Education System, it was tested in a different setting. The process of development, acceptability and applicability of nutrition education tools are summarised in Figure 1. Nutrition Education Tool?s Evaluation Questionnaire This questionnaire was developed based on previous literature to be able to evaluate the acceptability and applicability of nutrition education delivery tools.14, 17-18 Consented students initially completed their demographic profile which comprised of gender, race, living arrangement, study course and financial resources.
The NETEQ consisted of three sections with different questions each evaluating 1) conventional lectures (11 items with multiple choices response), 2) brochures (8 items – ranging from very unsatisfactory to very good) and 3) text messages via SMS (4 items – ranging from very unsatisfactory to very good). The survey on the conventional lectures focused on the level of understanding towards the contents, suitability of illustrations included in the slides and acceptability of the information viewed. Meanwhile, questions on the brochures asked about the contents, languages, frequency of brochure usage and the illustrations utilised. The final section of this questionnaire focused on the four criteria focusing on the contents, languages, time receiving of SMS, frequency of SMS received.
Ethical Approval
Ethical approval was granted by the Institute for Health Behavioral Research (IHBR), Clinical Research Centre (CRC) and Ministry of Health Research and Ethics Committee (MREC), Malaysia. Apart from that, institutional approvals from the selected universities were also sought prior to the data collection process. Permission to use the latest MDG 2010 was approved by National Coordinating Committee on Food and Nutrition (NCCFN), Nutrition Division, Ministry of Health Malaysia.
Statistical analysis
The results of the questionnaire were analysed by using SPSS 16.0 utilising descriptive statistics for all demographic characteristics and responses of acceptability and applicability of nutrition education delivery tools. Findings were presented as mean, standard deviation (SD), frequencies and percentages. A value of p<0.05 was considered statistically significant.
RESULTS
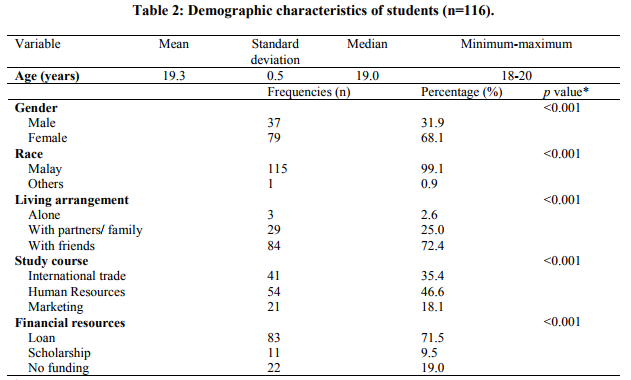
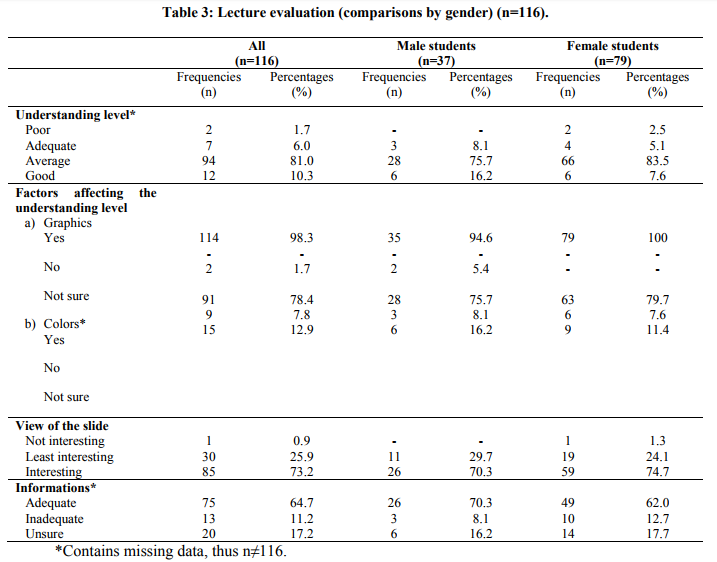
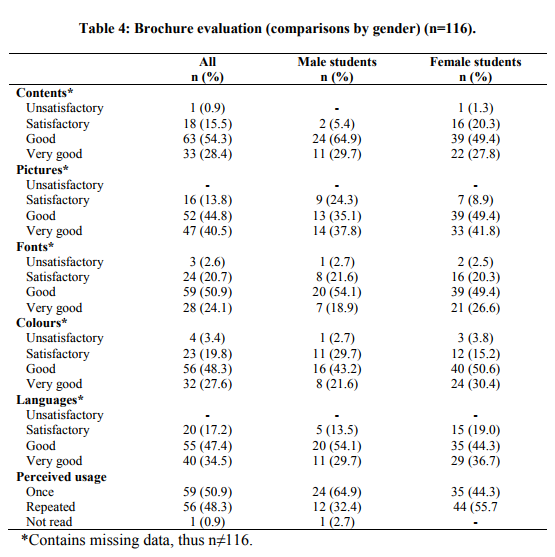
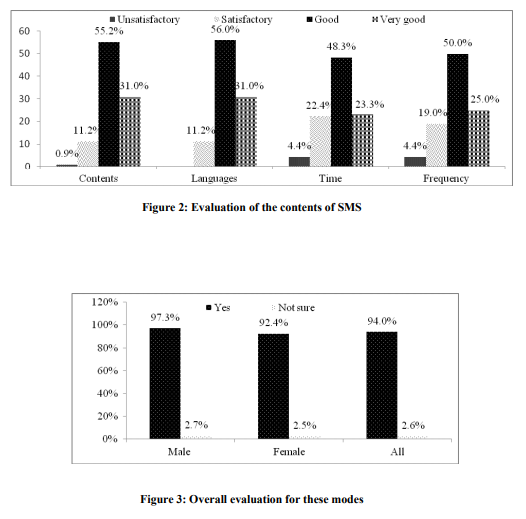
A total of 116 undergraduates participated in this investigation. Overall, the average age of the participants was 19.3 ± 0.5 years, ranging from 18 to 20 years. The average BMI of the group was 22.3 ± 4.7 kg/m2 with the majority of the respondents being female (68.1%). Most students were living in the dormitories with their friends (72.4%), while 25.0% were living with their family and only 2.6% reported to be living alone. Further details on demographic characteristic were shown in Table 2. The analysis of the data collected is shown in Table 3. In measuring understanding level of the slides, the majority of male (91.9%) and female students (91.1%) rated the slides as comprehensible (average to good). The slide contains several tables, however ten out of 116 students expressed their lack of understanding on the tables‘ contents presented. The respondents also preferred short sentences (48.3%) and requested more figures to be included in the slides (37.9%) to facilitate their understanding. Most of the respondents agreed that the graphics (98.3%) and colours (78.4%) helped improve their comprehension of the lecture delivered. About 18.1% of them suggested using combination of all colours. Overall, both genders (male=70.3%, female=74.7%) ranked the presentation as ?interesting?. In terms of information evaluation, the majority (64.7%) ranked the information included as adequate. Most of the respondents ranked the brochures to be at least ?good? with regard to the contents (82.7%), pictorial graphics (85.3%), fonts (75.0%), colours (75.9%) and languages (81.9%) used. Female students tend to read the brochures more than once compared to male students who inclined to read them only once. Unfortunately, one out of 116 respondents planned not to read them at all. Further details on brochure evaluation are shown in Table 4. In order to evaluate the text messaging system via SMS, the results indicated its acceptability and adequacy which most of students rated them at least as “good” with regard to the contents (86.2%) and languages (87.0%) used. Respondents were also requested to rate the delivery time of text messages via SMS at 10 a.m. as well as frequency of receiving SMS for once a week on a scale of good to very good. These two criteria received overall good rating, ranging from good to very good (time=71.6%, frequency=75.0%) (Figure 3). Overall, most of the respondents (94.0%) considered that information from the Malaysian Dietary Guidelines 2010 delivered in different ways is able to enhance their knowledge with regard to selecting the most appropriate diet and healthy lifestyle (Figure 4). Result of the evaluation for combination delivery tools has higher percentage in providing new knowledge compared to individual evaluation in conventional lecture, brochures or SMS.
DISCUSSION
The results of this study generally indicated that respondents were satisfied with all three newly developed nutrition education delivery tools. There may be several reasons for this situation. The variety of tools used in delivering such education (i.e. conventional lectures, brochures and SMS) could have been interesting and attractive. Previous studies have demonstrated that providing class-based nutrition intervention present the positive changes in soft drink and milk consumption and fruit and vegetable consumption notably among this students‘ population.10, 19 On the other hand, class based nutrition intervention was also applied in other population such as children which provide a positive impact on nutrition knowledge, attitude and practice of primary school children.20 Thus, using this conventional lecture as one of delivery tools may be an effective approach to promote healthy eating in a college setting. In order to enhance students‘ memory and understanding, useful written information could be given to them via the brochures and this written educational material is frequently used by healthcare professionals.21 The use of printed education materials is more efficient than oral language since readers can control the speed at which they read and comprehend the information.22 Other than that, written education materials are economical, can reinforce oral instruction and are the preferred form of education by most clients.23 Another finding that should be highlighted in our study is perceived usage of the brochures. We found that female students tend to read the brochures more than once compared to male students and only one student planned not to read them at all. This might be due to female students being more interested in reading and memorising compared to male students.24 Moreover, the nature of male students who prefers more on something technical such as web sites and video games while females like reading in comparison to video games.25 Hence, these additional tools can also be expected to be another effective tool in delivery of MDG 2010. Several studies have recommended the exploration of another interactive delivery channel through mobile telephone SMS to deliver information.26-27 One of our delivery tools used this method because these young adults frequently use mobile phone as their primary means of communication.28 Our results showed that this tool was positively accepted in terms of the contents, languages, timing and frequency of SMS delivery. A recent review by Fjeldsoe, Marshall and Miller 29 has suggested that weekly SMS-delivered interventions have positive short-term behavioural outcomes among healthy adults, patients with bulimia nervosa, diabetic patients and hypertension. 30-33 Another investigation also showed that intervention delivery through SMS may be more cost effective than other telephone or print-based interventions and has proven to be an effective tool to deliver regular alerts and reminders to achieve the desired goals in diabetic patients. 11, 34-35
The information delivered through nutrition education tool was adequate and clearly understood. A study by Joshi and co-investigators among patients with ureteric stents revealed that they dissatisfied with the information in booklet which is complex, inadequate, did not consider patients‘ needs and expectations as well as includes technical details.13 Therefore, health information delivered must be accurate, relevant to the target population and based on current practice standards.14 Overall, the information presented new Malaysian food pyramid as a main component in MDG 2010, healthy eating and balanced diet with performing physical activity through 13 key recommendations. During our observation, the term ?serving size? was not understood by almost all students. This might due to their background of study which is from a nonhealth science based. A study by Sajwani and comembers found that health science students had a superior level of knowledge on health issues regarding diet, lifestyle and exercise compared to non-health science students.36 As such, by providing nutrition education with adequate information on MDG 2010 through these three modes, it might promote positive changes on their dietary pattern and physical activity behaviours crucially among non-health science students. Mostly, respondents preferred short sentences with graphics in slides and brochures. Graphics may refer to any visual presentation of information such as pictures, charts, lists or graphs. According to Clayton graphics can be used to bridge language barriers, reduce the amount of text to read, emphasise key information and provide step-bystep directions.14 Most of the respondents in this study agreed that the graphics included in conventional lectures became a factor in affecting their understanding level. They also ranked the graphics provided in the brochures to be at least good. It is due to the graphics included which are simple, realistic, relevant and focus on students‘ actions.37 Pictorial usage in health education has been also shown to increase attention, comprehension, recall of what was explained and adherence to health recommendations.38 A study by Shankar and co-researchers reported that the role of pictures in such intervention had contributed to; 1) engagement, 2) comprehension, 3) information retention and 4) behaviour change which kept their attention focused on the information presented during the sessions.39 Employing appealing pictures accompanied by simple text is therefore better remembered than the presentation of text alone.38 Thus, the pictorial usage served as an important element in both the brochures and slides which are more likely to attract people‘s attention. The use of colours in both brochures and slides also play a part in adding quality to the nutrition education tool. A study by Ruzita and co-workers found that a combination of all colours in both slides and brochures similarly contribute as the important factors in increasing their attention and comprehension.18 Thus, applying the appropriate colours seemed to be accepted as the way to gain attention. We also found that respondents gave at least ?good? ranking for the fonts used in the brochures while layout in the slides was ranked as ?interesting?. These two criteria refer to the organisation and print of the health information. This finding could be because of font‘s sizes with 12-point Arial presented in the brochures and layout in the slides was making them easy to read and understand. According to Clayton the fonts should include at a minimum of a 12-point Serif font such as Times New Roman to facilitate reading and comprehension.14 Thus, the more eyes appealing the health information with the adequate colours, fonts and layout the more individuals are likely to review the education material.14 Although our study managed to recruit a large number of respondents, several drawbacks still exist. Firstly, the sample was rather imbalanced between genders due to the recruitment of more females over males as respondents; the results were thus heavily biased toward the females. This is due to higher proportion of female students, a common trend in the universities in our country.40 Secondly, this study evaluated the acceptability and applicability of nutrition education delivery modes. Therefore, the measure of improvement regarding nutrition knowledge and effectiveness of using the nutrition education delivery tools were unknown. Future studies should evaluate the actual effectiveness of these newly developed nutrition education delivery tools on changes of dietary habits and physical activities in longitudinal studies. As a conclusion, this newly-developed nutrition education delivery tools were accepted among this population. Acceptability and applicability for this nutrition education delivery tools were found to be accepted by the university students through the evaluation regarding to the contents, graphics, and languages. A combination of these three tools seemed to be more accepted in as a package of nutrition education compared to be used on their own. Thus, they can be used as an effective way to promote and improve students‘ dietary habits and lifestyle during university life.
ACKNOWLEDGEMENT
The authors would like to express their gratitude to Assoc. Prof. Dr. Ahmad Shukri Yazid, Dean of Faculty of Business Management and Accountancy, Mrs. Zaharah Dzulkifli, Head of Department Management and all first year and second year students of the Faculty of Business Management and Accountancy, UniSZA who have been instrumental in this study. The researchers are also grateful to the National Coordinating Committee on Food and Nutrition, Ministry of Health, Malaysia for their permission to use Malaysian Dietary Guidelines 2010 in this study. Assistance in data collection by Ms Noor Salihah Zakaria and Ms Nor Shahirah Mansor are highly appreciated.
References:
1. National Coordinating Committee of Food and Nutrition (NCCFN). Malaysian Dietary Guidelines. Ministry of Health Malaysia, Kuala Lumpur, 2010.
2. Norimah AK, Hwong CS, Liew WC, Ruzita AT, Siti Sa‘adiah HN, Ismail MN. Messages of the newly proposed Malaysian Dietary Guidelines (MDG): Do adults in Kuala Lumpur understand them? Mal J Nutr 2010;16:113-123.
3. Suzana S, Azhar Y, Fatimah A. Association between dietary fibre and cancer: A case control study. Mal J Nutr 2004;10:1173- 1182.
4. Fung TT, Hu FB, Pereira MA, Liu S, Stampfer MJ, Colditz GA, et al. Whole-grain intake and the risk of type 2 diabetes: a prospective study in men. Am J Clin Nutr 2002;76:535-540.
5. Liu S, Manson JE, Lee IM, Cole SR, Henneken CH, Willett WC, et al. Fruit and vegetable intake and risk of cardiovascular disease: the Women‘s Health Study. Am J Clin Nutr 2000;72:922-928.
6. Chourdakis M, Tzellos T, Papazisis G. Eating habits, health attitudes and obesity indices among medical students in northern Greece. Appetite. 2010;55:722-725.
7. Lollgen H, Bockenhoff A, Knapp G. Physical activity and all-cause mortality. An updated meta-analysis with different intensity categories. Int J Sports Med 2009;30:213- 224.
8. World Health Organization. Diet, nutrition and the prevention of chronic diseases. Report of a Joint WHO/FAO/Expert Consultation. WHO Technical Report Series 916. World Health Organization, Geneva, 2003.
9. Contento IR. The effectiveness of nutrition education and implications for nutrition education policy, programs and research: A review of research. J Nutr Educ Behav 1995;127:284-286.
10. Ha EJ, Caine-Bish N, Holloman C, LowryGordon K. Evaluation of effectiveness of class-based nutrition intervention on changes in soft drink and milk consumption among young adults. J Nutr 2009;50:1-6.
11. Krishna S, Boren SA. Diabetes selfmanagement care via cell phone: a systematic review. J Diabetes Sci Technol 2008;2:509- 517.
12. Franko DL, Cousineau TM, Trant M, Green TC, Rancourt D, Thompson D, et al. Motivation, self-efficacy, physical activity and nutrition in college students: randomized controlled trial of an internet-based education program. Prev Med 2008;369-377.
13. Joshi HB, Newns N, Stainthorpe A, Macdonagh RP, Keeley FX, Timoney AG. The development and validation of a patientinformation booklet on ureteric stents. BJU International 2001;88:329-334.
14. Clayton LH. Strategies for selecting effective patient nutrition education materials. Nutr Clin Pract 2010;25:436-442.
15. Cousineau TM, Franko DL, Ciccazzo M, Goldstein M, Rosenthal E. Web based nutrition education for college students: Is it feasible? J Eval Program Plann 2006;29:23- 33. 16. Perkins L. Developing a tool for health professionals involved in producing and evaluating nutrition education leaflets. J Hum Nutr Diet 2000;13:41-49.
17. Karupaiah T, Chee SS, Abdullah R. Devoloping a nutrition education package for Malaysian hemodialysis patients. J Renal Nutr 2001;11:220-227.
18. Ruzita AT, Rasyedah AR. Penerimaan masyarakat terhadap bahan pendidikan pemakanan bercetak. Mal J Nutr 2001;7:51- 60.
19. Ha EJ, Caine - Bish N. Effect of nutrition intervention using a general nutrition course for promoting fruit and vegetable consumption among college students. J Nutr Educ Behav 2009;41:103-109.
20. Shariff, ZM, Bukhari SS, Othman N, Hashim N, Ismail M, Jamil Z, et al. Nutrition education intervention improves nutrition knowledge, attitude and practices of primary school children: a pilot study. Int Electron J Health Educ 2008;11:119-132.
21. Clayton LH. TEMPtEd: Development and psychometric properties of a tool to evaluate materials used in patient education. J Adv Nurs 2009;65:2229-2237.
22. Redman B. The practice of patient education. 9 th ed. St. Louis, MO: Mosby, 2001.
23. Rankin SH, Stallings KD, London R. Patient education in Health and illness. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2005.
24. Rohana M. Ubah silibus tarik pelajar lelaki. Utusan Mealyu Press, 2010. 25. Silk KJ, Sherry J, Winn B, Keesecker N, Horodynski MA, Sayir A. Increasing nutrition literacy: testing the effectiveness of print, web site, and game modalities. J Nutr Educ Behav 2008;40:3-10.
26. Atkinson NL, Gold RS. The promise and challenge of eHealth Interventions. Am J Health Behav 2002;26:494-503.
27. Patrick K, Griswold WG, Raab F, Intille SS. Health and the mobile phone. Am J Prev Med 2008;35:177-181.
28. Koivusilta K, Lintonen T, Rimpela A. Orientations in adolescent use of imformation and communication technology: a digital divide by sociodemographic background, education career and health. Scand J Public Health 2007;35:95-103.
29. Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med 2009;36:165-172.
30. Hurling R, Catt M, DeBoni M, Fairley BW, Hurst T, Murray P, et al. Using Internet and mobile phone technology to deliver an automated physical activity program: randomised controlled trial. J Med Internet Res 2007;9: e7.
31. Robinson S, Perkins S, Bauer S, Hammond N, Treasure J, Schmidu U. Aftercare intervention through text messaging in the treatment of bilimia nervosa-Feasibility study. Int J Eat Disord 2006;39:633-638.
32. Rami B, Popow C, Horn W, Waldhoer T, Schober E. Telemedicine support to improve glycemic control in adolescents with type 1 diabetes mellitus. Eur J Pediatr 2006;165:701-705.
33. Marquez, Contreras E, Figuera Von Wichmann M, Guillen V, Figueras M, Balana M, et al. Effectiveness of an intervention to provide information to patients with hypertension as short text messages of reminders sent to their mobile phone. Aten Prim 2004;34:399-405.
34. Faulkner X, Culwin F. When fingers do the talking: a study of text messaging. Interacting Comput 2005;17:167-185.
35. Franklin VL, Waller A, Pagliari C, Greene SA. A randomized controlled trial of sweet talk, a text-messaging system to support young people with diabetes. Diabet Med 2006;23:1332-1338.
36. Sajwani RA, Shoukat S, Raza R, Sheikh MM, Rashid Q, Siddique MS, et al. Knowledge and practice of healthy lifestyle and dietary habits in medical and nonmedical students of Karachi, Pakistan. J Pak Med Assoc 2009;59: 650-655.
37. Doak CC, Doak LG, Meade CD. Strategies to improve cancer education materials. Oncol Nurs Forum 1996;23:1305-1312.
38. Houts P, Doak C, Doak L, Loscalzo M. The role of picture in improving health communication: a review of research on attention, comprehension, recall, and adherence. Patient Educ Couns 2006;61:173- 190.
39. Shankar S, Klassen AC, Mayer EG, Houts PS, Wang T, McCarthy M, et al. Evaluation of a Nutrition Education Intervention for Women Residents of Washington, DC, Public Housing Communities. Health Educ Res 2007;22:425-437.
40. Ministry of Higher Education. Statistics of Higher Education of Malaysia. Retrieved from http://www.mohe.gov.my/web_statistik/peran gkaan_2010.pdf, 2011.
APPENDIX 1
1) Pelbagaikan pilihan makanan dalam setiap hidangan anda untuk memastikan badan anda mendapat semua nutrisi yang diperlukan.
2) Kekalkan berat badan sihat (BMI 18.5 – 24.9) anda dengan mengimbangkan pengambilan makanan and melakukan aktiviti fizikal yang lazim.
3) Mulakan sekarang dengan melakukan aktiviti fizikal yang sederhana seperti bermain badminton, brisk walk, aerobik, sepak takraw, berbasikal dan berenang.
4) JANGAN ABAIKAN SARAPAN PAGI! Pilih bijirin yang tinggi serat seperti oat dan biskut yang rendah lemak dan mengandungi kurang gula dan garam
5) Makan banyak buah-buahan (sebiji oren + sepotong tembikai) and sayur-sayuran (2biji tomato + 1cawan bayam + 1cawan kubis) setiap hari. Pelbagaikan menu.
6) Pengambilan ikan secara kerap amat digalakkan. Daging lembu, ayam, itik atau telur perlulah diambil secara sederhana; makanlah kekacang setiap minggu.
7) Untuk individu yang ingin kurangkan berat badan, susu dan produk tenusu yang rendah lemak adalah pilihan yang sihat berbanding dengan susu penuh krim.
8) Makanlah di tempat yang menyediakan pilihan makanan yang sihat dan minta untuk kurangkan minyak, garam, gula dan lemak apabila memesan makanan.
9) Kurangkan makanan bergaram tinggi; ikan masin, telur masin, sayur jeruk, makanan ringan, sosej, nugget ayam, bebola daging and burger.
10) Kurangkan minuman bergula seperti minuman bergas, kordial, cendol and air batu campur. Pilihlah kuih atau kek yang mengandungi kurang gula.
11) Ingatlah, air yang hilang perlu diganti setiap hari untuk mengekalkan keseimbangan cecair dalam badan. Minum sekurang-kurangnya 8 gelas sehari.
12) Makan makanan and minum minuman yang bersih and selamat untuk mengelak terkena keracunan makanan. Amalkan kebersihan diri ketika menyediakan makanan.
13) Perhatikan maklumat pemakanan pada label makanan/ minuman semasa membuat pilihan seperti maklumat tentang jumlah tenaga dan nutrisi.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





