IJCRR - 8(22), November, 2016
Pages: 18-21
Print Article
Download XML Download PDF
RELIEVING THE TIE: CASE SERIES OF MANAGEMENT OF TONGUE-TIE
Author: Renganath M. J., Ramakrishnan T., Manisundar N., Vidya Sekhar, Ebenezer M., Sivaranjani P.
Category: Healthcare
Abstract:Aim: Ankyloglossia, which is also commonly known as tongue-tie, either partial or complete may lead to various difficulties and deformities that includes abnormal speech, mal-occlusion and inability in deglutination thus being an undesired problem in normal life activity. Various techniques like scalpel, laser, and electro-surgery have been performed for the past few decades in treating tongue-tie. Though, each techniquehas got their own advantages and disadvantages, all aimed at relieving the high muscle attachment to improve the movement of the tongue. Hence, scalpel have been preferred for treating the cases with ankyloglossia.
Case Report: This series of case reports of 2 cases with partial ankyloglossia, exhibiting speech difficulty along with restricted tongue movementswhich requires definitive treatment to correct the deformity.
Discussion: The outcome of the frenulectomy in the 2 cases using scalpel showed good healing with improved tongue movements than that of pre-operative movements thus achieving the primary objective of relieving the tongue-tie.
Conclusion: The clinical outcome following the surgical frenulectomy for the 2 cases treated by scalpel has shown better healing with improvement in tongue movements suggesting that surgical frenulectomy could be considered as the reliable technique for the treatment of ankyloglossia..
Keywords: Ankyloglossia, Tongue-tie, Surgical/scalpel frenulectomy, Speech defect
Full Text:
Introduction
Ankyloglossia (Tongue-tie) is defined as partial or complete fusion of the tongue with the floor of the mouth or the lingual gingiva due to an abnormally short, mid-line lingual frenulum, resulting in restricted tongue movement.1Tongue-tie may lead to various functional abnormalities that includes abnormal speech, mal-occlusion, inability to swallow the food which could entail difficulty in normal life activity of an individual.
Ankyloglossia may be partial or complete and may lead to the above mentioned problems. Although, both partial and complete ankyloglossia requires surgical correction, certain partial ankyloglossia, may not require treatment, which could be corrected by performing tongue movement exercises. Speech problems can occur as a major concern, when there is limited mobility of the tongue due to ankyloglossia. Therefore, a little correction or relieving of the highly attached lingual frenulum can lead to improvement and correction of the speech problems caused by tongue-tie.
This series of case report describes management of 2 cases with partial ankyloglossia, treated by means of surgical excision with scalpel and the potential outcome of the treatment showing enhanced tongue movement.
Case 1
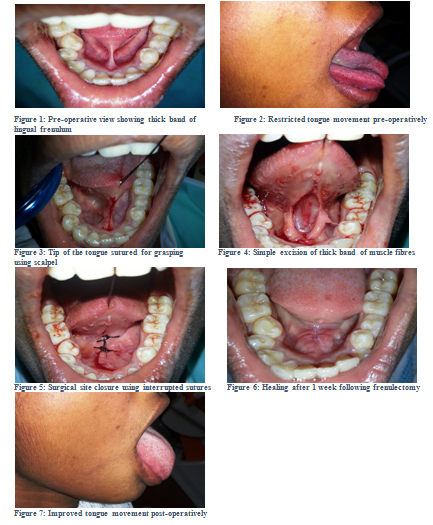
A 20 year old female patient reported to department of Periodontics, Adhiparasakthi dental college, Melmaruvathur, Tamilnadu, with the chief complaint of difficulty in moving her tongue freely which often causes speech difficulty in pronouncing certain words freely. On intra oral examination, the tongue exhibited limited movements due to high frenal attachment to the floor of the mouth [fig 1], leading to inability in movements like protrusion and lateral movements [fig 2]. It was diagnosed as partial ankyloglossia and so frenulectomy was planned by means of scalpel. Under local anaesthesia, bilateral lingual nerve block, the tongue was sutured at its tip using 3-0 silk suture material [fig 3] in order to hold or retract the tongue conveniently. Excision of the high frenulum muscle fibres was done by giving 2 incisions, with one on the upper and other on the lower border of the frenulum attachments [fig 4]. Following the excision of the muscle fibres, simple interrupted sutures were placed to close the surgically open site [fig 5] along with prescription of antibiotic regimen (Amoxicillin 500mg and Metronidazole 400 mg) thrice a day and analgesic (Acelofenac paracetamol) twice a day for five days. The sutures were removed 1 week following the day of surgery which showed excellent healing [fig 6] and the tongue movements were re-evaluated which showed better improvement in its movement in all the directions compared to the movements observed pre-operatively [fig 7]. Patient was advised to practice speech by reading and pronouncing consonants and sounds thatincludes “s, z, t, d, l, j, zh, ch, th, dg” to improve the pronunciations of difficult consonants.
Case 2
A 20 year old male patient reported to department of Periodontics, Adhiparasakthi dental college, Melmaruvathur, Tamilnadu, with the chief complaint of speech difficulty in pronouncing certain words freely. On intra oral examination, the tongue exhibited lack of protrusion and lifting movements due to high frenal attachment to the floor of the mouth and extending till the attached gingiva in relation to teeth 31 and 41 lingually. It was also diagnosed as partial ankyloglossia and frenulectomy was planned same as the case 1 by means of scalpel. Under local anaesthesia using bilateral lingual nerve block, frenulectomy procedure using scalpel was performed same as like case 1 and sutures was placed to close the surgical site. After a week, sutures were removed and tongue movements were re-evaluated, which showed improved tongue movements in all the directions. This patient was also advised to practice speech by continued reading by pronouncing the sounds “s, z, t, d, l, j, zh, ch, th, dg” same as like case 1to improve the pronunciations of difficult consonants.
Discussion
The tongue is a vital organ of important functions including deglutition, mastication, and speech. It also exerts a major influence on occlusion of the dentition, growth of the jaws, and enhances to maintain the facial form. In the infant, the normally mobile tongue is unconfined by teeth and thus extends outward between the maxillary and mandibular arches. During deglutition, the infant keeps the jaws parted whereas the tongue is placed between the occlusal gum pads to produce a vacuum for sucking.
During teeth eruption, the tongue remains confined within the oral cavity. At approximately 21/2 years of age, when all deciduous teeth have erupted and are in occlusion, the "infantile swallow" is replaced by the "adult swallow". In the adult swallow, the lips are closed, the teeth held in occlusion, and the tip of the tongue raised and pressed against the anterior portion of the palate, sealing the anterior portion of the mouth.
For unknown reasons, few individuals do not outgrow their infantile swallow and continue to swallow with their jaws apart. Any band or condition restricting freedom of motion of the tip of the tongue and preventing it from touching the anterior palate may interfere with the development of an adult swallow and perpetuate the infantile swallow, resulting in an open bite deformity.2
Ankyloglossia was also found associated in rare syndromes such as Van der Woude syndrome,3 X-linked cleft palate syndrome,4 Opitz syndrome5 and Kindler syndrome.6 Nevertheless, most ankyloglossias are observed in persons without any other congenital anomalies or diseases.
The major problem associated with the tongue-tie includes speech difficulty. The difficulties in pronunciationof consonants and sounds includes “s, z, t, d, l, j, zh, ch, th, dg”. 7 Here, both the patients came with the chief complaint of inability in pronouncing the above mentioned words due to restricted tongue movement.
Ankyloglossia can be classified based on Kotlow’s assessment:8
Class I: Mild ankyloglossia: 12 to 16 mm,
Class II: Moderate ankyloglossia: 8 to 11 mm,
Class III: Severe ankyloglossia: 3 to 7 mm,
Class IV: Complete ankyloglossia: Less than 3 mm
Where, class III and IV casesrequires definitive surgical correction because they the tongue’s movements are severely restricted in these cases. Hence, clinically acceptable, normal range of free tongue should be greater than 16 mm and a normal range of tongue movements exhibits as the tip of the tongue should be able to protrude outside the mouth; without clefting, and also the tip of the tongue should be able to sweep the upper and lower lips easily; without straining. When in retruded position, the tongue should not blanch the tissues lingual to the anterior teeth; and the lingual frenum should not create a diastema between the mandibular central incisors. If severe/complete ankyloglossia is present in an adult, there is usually an obvious limitation of the tongue protrusion, elevation and speech problems which can be improved following surgical intervention.9
There is continuing controversy over the diagnostic criteria and treatment of ankyloglossia.10 Literature reviews and various case reports in the past few decades have shown the benefits and clinical outcomes of various techniques like scalpel, laser, and electro-surgery for the treatment of tongue-tie. But all the techniques aimed at relieving the high muscle attachment to improve the movement of the tongue.
Here, for the 2 cases, surgical frenulectomy using scalpel was planned, since surgical excision of the muscle fibres thus relieving the frenulum was simple, easier as well as time consuming. The most expedient factor of electing scalpel over the other techniques like Laser, electro-surgery was because of the fact that the complete excision of the lingual frenulum muscle fibres could be achieved by means of scalpel rather than any other techniques. But caution should be taken while preferring scalpel in order not to traumatize the adjacent vital structures including lingual nerve, vein and sub lingual duct.
The outcome of the frenulectomy in the 2 cases using scalpel in one week post-operative review showed good healing without any post-operative complications. The tongue exhibited improved movements when compare to the movements observed pre-operatively. Thus the primary objective of relieving the tongue-tie has been achieved by the surgical frenulectomy.
Conclusion
Ankyloglossia in adults causing obvious limitation of the tongue protrusion, elevation and especially speech problems could be improved by surgical intervention. The clinical outcome following the surgical frenulectomy for the two cases presented here shown better healing with improvement in tongue movements. With the limitation of this case reports, it could be concluded that surgical frenulectomy remains one of the best and reliable technique for the management of tongue-tie. Further studies with large sample size should be done to support the beneficial outcomes of this technique.
Acknowledgement
The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
- American Academy of Periodontology. Glossary of Periodontal Terms. Chicago: American Academy of Periodontology; 2001:3.
- Tuerk, M., and E. C. Lubit, Ankyloglossia. Plastic reconstr. Surg., 1959: 24,271-6.
- Burdick AB, Ma LA, Dai ZH, Gao NN. Van der Woude syndrome in two families in China. J Craniofac Genet DevBiol 1987;7: 413-8.
- Moore GE, Ivens A, Chambers J, Farrall M, Williamson R, Page DC, et al. Linkage of an X-chromosome cleft palate gene. Nature 1987;326:91-2.
- Brooks JK, Leonard CO, Coccaro PJ Jr. Opitz (BBB/G) syndrome: Oral manifestations. Am J Med Genet 1992;43:595-601.
- Hacham-Zadeh S, Garfunkel AA. Kindler syndrome in two related Kurdish families. Am J Med Genet 1985;20:43-8.
- Messner AH, Lalakea ML. The effect of ankyloglossia on speech in children. Otolaryngol Head Neck Surg 2002;127:539-45.
- Kotlow LA. Ankyloglossia (tongue-tie): A diagnostic and treatment quandary. Quintessence Intl 1999;30:259-62.
- Chaubal TV, Dixit MB. Ankyloglossia and its management. Journal of Indian Society of Periodontology. 2011 Jul 1;15(3):270.
- Messner AH, Lalakea ML. Ankyloglossia: controversies in management. Int J Pediatr Otorhinolaryngol. 2000;54 (2/3):123- 31.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





