IJCRR - 9(13), July, 2017
Pages: 62-65
Date of Publication: 03-Jul-2017
Print Article
Download XML Download PDF
Prevalence of Oral Submucous Fibrosis Among Betel Nut Chewers Dental Patients of Patna
Author: Tanoj Kumar, Mobeen Khan, Chandra Prakash Gupta, Shah Faisal, Nazish Akhtar, Divyanshu Shrivastava
Category: Healthcare
Abstract:Background: Oral Submucous Fibrosis (OSMF) is premalignant condition having high malignant transformation rate and increased risk of oral squamous cell carcinoma which itself accounts for 40% deaths due to malignancy across the world.
Objective: To study the prevalence of OSMF among betel nut chewers in north Indian population. Methods: A total of 320 subjects consisting of 246 males and 74 females Dental patients of Patna were selected. The subjects were divided into two groups. The first group was control group consisting of 160 subjects including 123 males and 37 females who didn't had the habit of betel nut chewing. Another group included betel nut chewers with same no of subjects as that of control group. All participants were screened for presence of OSMF by first 2 authors independently according to the WHO prescribed coloured atlas, clinical examination and history. Results: Prevalence of OSMF was 75% among betel nut chewers. Males were more affected (70%) than the females. The maximum no of cases reported were in the age group of 30-40 years.
Conclusion: Betel nut chewing can be considered to be a harmful habit and necessary public health measures should be taken to eradicate this habit.
Keywords: OSMF, Betel nut chewers, Premalignant condition
DOI: 10.7324/IJCRR.2017.91311
Full Text:
INTRODUCTION
Oral submucous fibrosis (OSMF) is a premalignant disorder with a high malignant potential of 12-18%.It causes significant morbidity. After getting transformation into squamous cell carcinoma (SCC), it leadsto mortality.Oral cancer accounts for up to 40% of total malignancies in Asia. Tobacco smoking and betel quid chewing containing tobacco are considered to be the major risk factors for oral cancer, whereas betel quid without tobacco has been also reported to significantly increase the risk for oral cancer in some studies. OSMF found to cause oral cancer 19.1 times more likely than normal individuals.1


The initial clinicalpresentation of OSMF includes inflammation. It is followed by hypovascularity and fibrosis observed as blanching of the oral mucosa characterized with a marble-like appearance. It may be localized, diffuse, or reticular.However, in some cases, small vesicles may develop that subsequently rupture and form erosions.2 In the later advanced stage of OSMF, a fibrotic band that reduces mouth opening is characteristic feature. It causes further problems in maintaining oral hygiene, proper speech, normal mastication, and swallowing. Formation of fibrous bands in the lip give rise to thickening and rubbery appearance .Other clinical features of advanced OSMF include the absence of puffed-out appearance of cheeks which is observed usually when a patient blows a whistle. Fibrosis of tongue and mouth affect tongue movement and cause depapillation and blanching of mucosa.3
OSMF is found to be associated with the chewing of areca nut (betel nut). This habit is prevalent in South Asian populations but being recognized nowadays also in some parts of Europe and North America. The combination of areca nut and tobacco has led to a sharp increase in the frequency of OSMF.2Betel is found to contain areca nut (Areca catechu), fewfresh leaf of betel pepper (Piper betle), some spices, and little calcium hydroxide (lime). Chewing tobacco or guthka gained a lot of popularity, and betel chewers were found to use guthka quite frequently. However, guthka officially banned from the Indian market recently.4-5Despite this chewing tobacco-containing betel quid hasreported to become one of the most popular bad habits in South Asia.6 Betel is now found widely in the Western world also.OSMF subjects are usually younger and have reported shorter histories of chewing as compared to chewers without OSMF.
The present study was conducted to evaluate the prevalence of OSMF among betel nut chewers in different age groups among north Indian population.
METHODS AND MATERIALS
A total of 320 subjects consisting of 246 males and 74 females Dental patients of Patna were selected for the study after getting their informed consent. The subjects were divided into two groups. The first group was control group consisting of 160 subjects including 123 males and 37 females who didn’t had the habit of betel nut chewing. Another group included betel nut chewers with same no of subjects as that of control group.
The subjects aged between 20 to 60 years were included in the study. Inclusion criteria for subjects being included in betel nut chewers group consisted of habit of chewing areca nut/pan/gutkha for more than3 year, with a frequency of more than 5 times per day.The subjectswith reduced mouth opening due to other reasons like odontogenic infections and Temporomandibular joint disorders and subjects having habit of tobacco smoking were excluded from the study.
All participants were examined for presence of OSMF independently according to the WHO prescribed coloured atlas, clinical examination and history. The examiner was not blinded about the chewing habit of the study subject. In the OSMF patients, a detailed history was obtained including duration, information regarding type and frequency of the chewing habit in study subject.
Presence of blanching and fibrous bands was observed for each subject. Interincisal distance was recorded between maxillary and mandibular central incisors with use of vernier calipers. An interincisal distance of >30 mm was considered normal and <30 mm was considered to be reduced mouth opening.The data obtained was analyzed by using SPSS (Statistical Package for Social Services) 16.5 version.
RESULTS
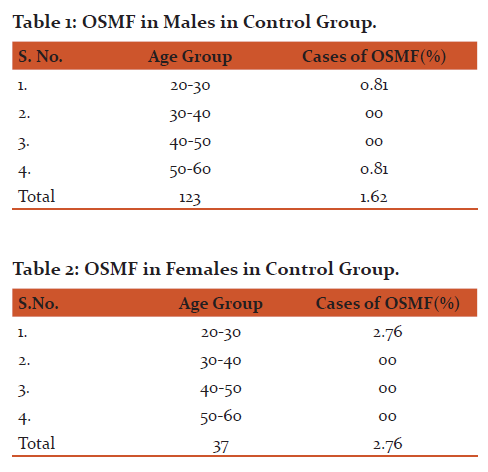
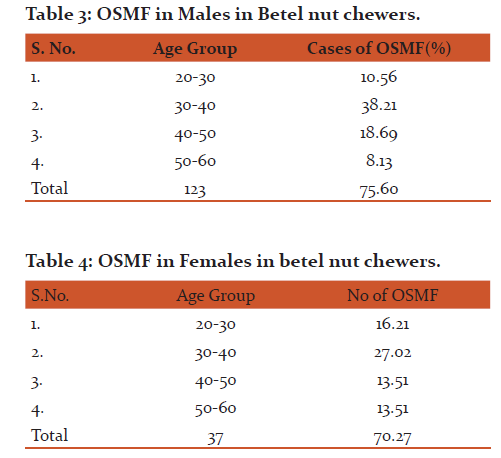
The control group consisted of 123 males and 37 females. Only 1.62% cases of OSMF noticed in male subjects(Table 1) while 2.76% cases of OSMF detected in female subjects(Table 2).
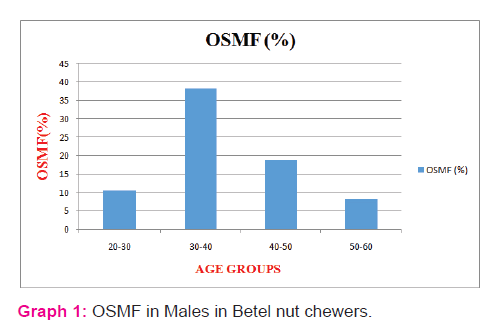
The group consisting of betel nut chewers included 123 males and 37 females. In male subjects, 75.60% cases of OSMF were observed. Maximum no cases were observed in age group of 30-40 years accounting 38.21% cases. It was followed by 18.69 % cases as reported in 40-50 years of age. Among subjects of 20-30 years age group 10.56 % cases were reported. While least no of cases (8.13%) was observed in the age group of 50-60 years.(Table 3, Graph 1)
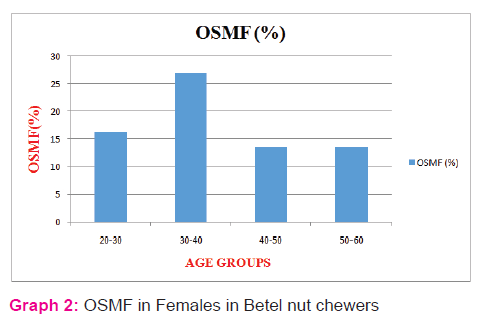
In female subjects 70.27% cases of OSMF was observed. Maximum no cases were observed in age group of 30-40 years accounting 27.02% cases. It was followed by 16.21 % cases as reported in 20-30 years age group. Among subjects of 20-30 years age group 10.56 % cases were reported. While least no of cases (13.51%) was observed in the age group of both 40-50 years and 50-60 years.(Table 4, Graph 2)
DISCUSSION
Our study found a prevalence of 75% OSMF among habitual betel nut chewers of the Patna Dental patients. Previous reports fromother parts of India and neighbouring Asian countries showed similar prevalence. Ranganathan et al found that 69% of OSMF patients were gutkha chewers in a study sample of 185.7But, Murti et al in their publication mentioned that 98% of OSMF patients were reported to use areca nut either alone or in combination with tobacco.8Recent increase in gutkha chewing with areca nut is due to the frequent availability of attractive, easy portability of small, colourful gutkha packets.
In the present study males were dominating, 123 (73%) OSMF out of 160 were male. The male to female ratio was 2.9:1. In a previous study conducted in Mumbai by Sirsat9 and Khanolkar, it was reported that the male to female ratio was 1:1. Similarly Wahi et al11 found a male: female ratio of 2:1. Later on Shah and Sharma12 had same study with same results like earlier studies on OSMF subjects.
However, in the present study, males were found to be more dominantly affected, as they were using gutkha and other related products more frequently because of easy availability of gutka at all the working places where as females who are more conscious about their health as well as esthetic value, usually felt uncomfortable in asking the vendors to provide the gutkha products. As a possibility it may be one of the reasons, which might be leading cause for a high male to female ratio.
In our study youngest patient was 20 years of age where as the oldest patient was 57 years. Majority of the OSMF cases belonged to 30-40 years of age group. Previously Sirsat and Khanolkar13 found that a majority of OSMF cases reported to the age group of 20-40 years of age. Sinor et al14 reported that 79 per cent of the OSMF cases were below the age of 35 years and majority of cases were in 25-44 years of age group. Shah and Sharma11 in their study from AIIMS also found the majority of cases between 21-40 years of age group. Our study also indicated that most of the younger adults were suffering from OSMF. Usually in India, only married adults are among daily consumers of areca nut. However, in the the recent years, with the availability of attractive, nicely packed gutkas and vigorous media advertisements, consumption of gutkha and panmasala by younger individuals has outs urged.
CONCLUSION
The present study shows that prevalence of OSMF is high (75%) among the betel nut chewers. OSMF is premalignant condition having high malignant transformation rate and increased risk of oral squamous cell carcinoma which itself accounts for 40% deaths due to malignancy across the world. Hence it can be concluded that there is need for public health awareness regarding the dangerous outcomes of habitual betel nut chewing.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in reference of this manuscript. The authors are grateful to authors / editors / publishers of all those articles, journal and books from where the literature for this article has been reviewed and discussed.
References:
1.Cox S. Oral cancer in Australia – risk factors and distribution. Ann R Australas Coll Dent Surg. 2000;15:261–263.
2. Haider SM, Merchant AT, Fikree FF, Rahbar MH. Clinical and functional staging of oral submucous fibrosis. Br J Oral Maxillofac Surg. 2000;38(1):12–15.
3.Chaudhry K. Is pan masala-containing tobacco carcinogenic? Natl Med J India. 1999;12(1):21–27.
4. Gupta PC, Sinor PN, Bhonsle RB, Pawar VS, Mehta HC. Oral submucous fibrosis in India: a new epidemic? Natl Med J India. 1998;11(3): 113–116.
5. Roy R. Taxes make cigarette firms huff and puff. The Sunday Times of India, Mubai, 12 (17): February 3, 2002, p 1.
6. Heck JE, Marcotte EL, Argos M, et al. Betel quid chewing in rural Bangladesh: prevalence, predictors and relationship to blood pressure. Int J Epidemiol. 2012;41(2):462–471.
7. Ranganathan K, Devi MU, Joshua E, Kirankumar K, Saraswati TR. Oral submucous fibrosis: a case control study in Chennai, South India. J Oral Pathol Med. 2004;33(5):274e277.
8. Hazarey VK, Erlewad DM, Mundhe KA, Ughade SN. Oral submucous fibrosis: a study of 1000 cases from central India. J Oral Pathol Med. 2007;36(1):12e17
9. Sirsat SM, Khanolkar VR. Submucous Fibrosis of the Palate and Pillars of the Fauces. Indian J Med Sci 1962;16:188-97.
10. Wahi PN, Kapoor VL, Luthra UK, Srivastava MC. Submucous Fibrosis of the oral cavity: Studies on Epidemiology. Bull WHO 1966;35:793-9.
11. Shah N, Sharma PP. Role of chewing and smoking habits in the etiology of oral submucous fibrosis: A case control study. J Oral Pathol Med 1998;27:475-9.
12. Sirsat SM, Khanolkar VR. Sub mucous fibrosis of the palate in diet. Pre conditioned Wister rats: Induction by local painting of capsaicin-an optical and electron microscopic study. Arch Pathol 1960;70:171-9.
13. Sinor PN, Gupta PC, Murti PR, et al . A case control study of oral submucous fibrosis with special reference to the etiologic role of areca nut. J Oral Pathol Med 1990;19:94-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





