IJCRR - 5(8), April, 2013
Pages: 118-125
Date of Publication: 25-Apr-2013
Print Article
Download XML Download PDF
MORPHOMETRICAL STUDY OF MENISCI OF HUMAN KNEE JOINT
Author: Ashwini C. , Nanjaiah C.M. , G.S. Saraswathi, N.M. Sham sundar
Category: Healthcare
Abstract:Introduction: The knee is the largest synovial joint in our body. Among the different ligaments of knee joint, menisci are a pair of fibro cartilaginous plates situated within the knee joint on the tibial condyles. Lubrication, proprioception, joint stabilization, load transmission are the major functions of the knee meniscus. Variations of form and in particular of thickness and width of menisci can determine the possibility and the kind of injury. Meniscal replacement is required in cases of severe loss of meniscal issue or degenerated. The correct size of the allograft is likely to be critical for successful healing and functionality. Objective: 1) To determine the thickness, width and circumference of the menisci of human knee joint 2) To measure the distance between anterior and posterior horn of the menisci of human knee joint. Material and Methods: 50 menisci of 25 knees of the formalin fixed adult human cadavers were dissected and studied in the department of anatomy, JSS Medical College, Mysore. The knee joints included 13 right and 12 left specimens. A slide caliper is used to measure the distance between anterior horn and posterior horn of the menisci and to measure the thickness and width in anterior 1/3rd, middle1/3rd and posterior 1/3rd of the menisci. Outer circumference and inner circumference is measured by non elastic cotton thread. Results: The peripheral length and inner border length of medial meniscus was more than that of the lateral meniscus. Posterior third of the medial and lateral menisci was the thickest part compared to anterior and middle thirds. The distance between the anterior and posterior horns of the medial meniscus was significantly more than the lateral meniscus. The individual analysis of each meniscus showed that the posterior third was the widest part than the anterior and middle thirds.
Keywords: Knee, Meniscus, Thickness, Length
Full Text:
INTRODUCTION
The knee is the largest synovial joint in the body. It consists of femoro-patellar, medial and lateral tibio-femoral articulations which form a complex 'hinge' variety type of joint. This arrangement offers a fulcrum for propulsion, and allows the limb to bear and transmit the body weight. Because of the wide range of its mobility it has more tendencies for instability, to counter this tendency, a complex ligament arrangement has evolved1 . Among the different ligaments of knee joint, menisci are a pair of fibro cartilaginous plates situated within the knee joint on the tibial condyles. Lubrication, proprioception, joint stabilization, load transmission are the major functions of the knee meniscus. Among many types of meniscal anomalies reported, discoid meniscus is the most common entity. Identification of discoid meniscus is clinically important because of its high prone to injury than the normal meniscus. Knowledge of the dimensions of the normal meniscus could help to differentiate between the discoid meniscus and a normal meniscus. This is important for planning surgical interventions in the knee joint. Variations of form and in particular of thickness and width of menisci can determine the possibility and the kind of injury2,3 . It is observed by Fairbank that the removal of the meniscus lead to degenerative changes in the knee joint in the long term4 . Nowadays the meniscus is repaired instead of removed, but this treatment is only feasible when the meniscus tissue is otherwise of good quality. Meniscal cartilage can be conserved by replacing or by re-growing the cartilage which must be accompanied by measurement techniques to determine meniscal size. So the correct size of the allograft is likely to be critical for successful healing and functionality. With this clinical perspective, the aim of our work is to determine the thickness of the menisci, width of the menisci, circumference of the menisci and to measure the distance between anterior and posterior horn of the menisci.
OBJECTIVES
1) To determine the thickness, width and circumference of the menisci of human knee joint
2) To measure the distance between anterior and posterior horn of the menisci of human knee joint
MATERIAL AND METHODS
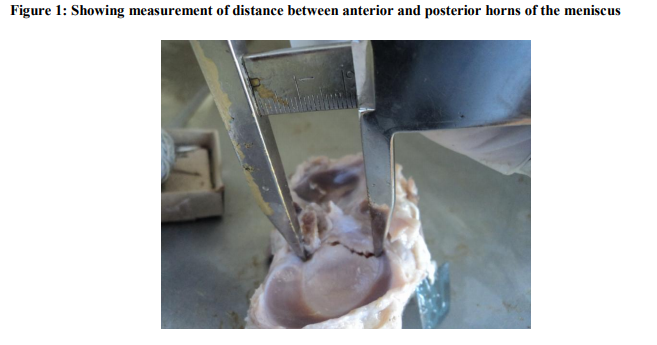
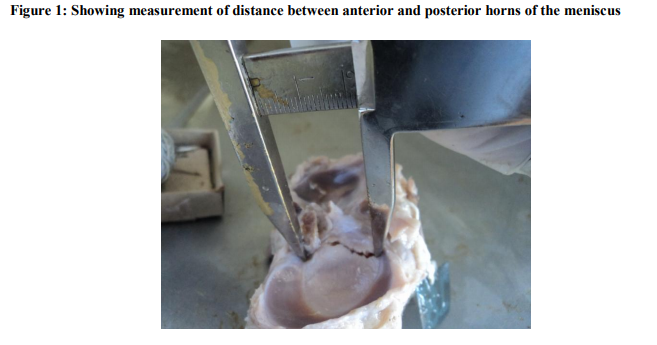
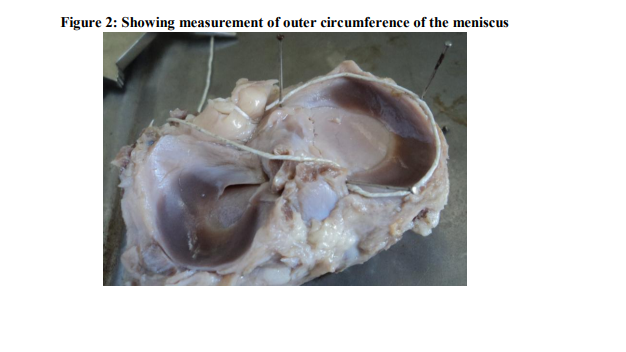
50 menisci of 25 knees of the formalin fixed adult human cadavers were dissected and studied in the department of anatomy, JSS Medical College, Mysore. The knee joints included 13 right and 12 left specimens. All menisci that showed any structural change which prevents its morphometric analysis such as injuries or advanced degenerative changes were excluded. After the removal of skin and the muscles surrounding the knee joint, joint cavity is opened anteriorly by a vertical incision on joint capsule and by dividing the patellar and collateral ligaments horizontally. Menisci are exposed clearly by cutting the cruciate ligaments and then the tibial condyles with menisci are disconnected from the femur. The data were collected with the aid of sliding callipers, and were recorded manually. The collection followed the following protocol in both menisci (lateral and medial): the distances between the anterior and posterior horns were measured using the sliding calipers, which was placed between the apex of the anterior horn and the apex of the posterior horn. (Figure1) Then, the peripheral lengths of the menisci were measured with the non- elastic cotton thread. (Figure 2) For this, a piece of thread was placed across the outer edge of the meniscus from the apex of the anterior horn to the apex of posterior horn. The thread which placed along the periphery of the meniscus was held in place with metallic pins. The length of this thread from the most anterior part of the insertional area to the most posterior part was measured and was called “peripheral length”. In the same way, the inner free border length was measured by keeping the thread at the inner free edge. Next, the thread length was measured using sliding calipers. To measure the thickness of menisci, firstly we determined its length. Then the menisci were divided into 3 equal parts using the thread and the parts are called anterior1/3rd, middle1/3rd and posterior1/3 respectively. The thickness and width of the menisci was measured with the vernier caliper. The measurements of the thickness and width were done at the midpoint of the above mentioned 3 parts. Then thickness values were noted by measuring at midpoint between outer and inner circumference.
RESULTS
There were some statistically significant morphometrical differences between medial and lateral meniscus. The peripheral length of medial meniscus (90.12±8.0.mm) were not significantly more than (p>0.05) that of the lateral meniscus (83.28 ± 7.46mm) where as inner border length of medial meniscus (59.96±8.55mm) were significantly more than (p<0.05) that of the lateral meniscus (49.0 ± 5.492mm).Related to the thickness of meniscus at the midpoint of its width, the posterior third of the medial and lateral menisci was the thickest part compared to anterior and middle thirds. There was no statistically significant difference found between the posterior, anterior and middle thirds (p>0.05) of medial menisci. A statistically significant difference was observed (p<0.05) among the anterior, middle and posterior thirds of lateral meniscus Comparing the average values of thickness of middle third of medial meniscus with the values of lateral meniscus, the statistically significant difference (p=0.043) was observed. There was no statistically significant difference found on comparing the anterior and posterior thirds of thickness between medial and lateral menisci. The individual analysis of each meniscus showed that the posterior third (11.28±2.09mm) was the widest part of the medial meniscus (p=0.00, p=0.00) than the anterior (6.52±1.29mm) & middle thirds (6.66 ±1.11mm). There was no statistically significant difference found between the anterior and middle thirds (p>0. 05) (Table 1). In the lateral meniscus the posterior third part (9.36 ± 1.19mm) was the widest compared to the anterior third (8.08 ± 1.14mm) and the middle third parts (8.52 ± 2.12 mm). It was found that anterior third was more than that the posterior third and it was statistically significant (p<0.05). There was no statistically significant difference found between the anterior and middle thirds and middle and posterior thirds (Table 2).
The distance between the anterior and posterior horns of the medial meniscus (21.32+3.7 mm) was significantly more than (p=0.001) the lateral meniscus (6.8 + 1.97mm). Independent t-test and Repeated Measures ANOVA were performed for the comparison of variables. Two tailed p-values < 0.05 (?= 0.05) were considered significant. The Epi info 3.43 program was used for statistical analyses. Data were presented as mean ± SD. b
DISCUSSION
The data referring to the dimensions of semilunar cartilages are varied. Braz & Silva (2010) in a generalized description of the morphometry of menisci, mention that the average thickness of outer circumference of medial and lateral menisci were 5.88 mm & 5.46 mm respectively5 . Almeida et al. in their study states that average value of thickness of medial and lateral menisci were 5.71mm and 5.19 mm respectively2 . In our study we measured the thickness of the meniscus at three regions anterior third, middle third & posterior third. The midpoint of that region was selected to measure thickness. With the best of our knowledge there are no literatures available measuring the thickness at these points. We observed that the posterior third (1.8 ± 0.78 mm) of the medial meniscus was the thickest part followed by middle third (1.77 ± 0.56 mm) & anterior third (1.54 ± 0.78 mm) was the thinner. This difference among the anterior, middle and posterior thirds of medial meniscus was of no statistical significance (p>0.05). With regard to the thickness of the outer circumference of the medial meniscus, Almeida et al. in their study observed that medial menisci was the thinnest at posterior third followed by anterior and middle thirds in contrast to Braz & Silva who observed the middle third was the thickest compared to other two points5 . (Table 3 &4) In our study we found that the posterior third (2.06 ± 9.3 mm) of the lateral meniscus was the thickest part (p<0.05) followed by middle third (1.76 ± 0.81 mm) & anterior third (1.41 ± 0.51 mm) was the least. A difference statistically significant was observed (p<0.05) among the anterior, middle and posterior thirds of lateral meniscus. Comparing the thickness of the middle third of both the menisci, it was observed that the thickness of the middle third of the medial meniscus was thicker than that of the middle third of the lateral meniscus. This explains the higher incidence of injuries in the medial meniscus. There was no statistically significant difference found on comparing the thickness of anterior and posterior thirds between medial and lateral menisci. In a study on the location of the meniscal injuries , Rico and Ayala (1997) observed that the medial meniscus was more commonly affected and topographical lesions were more frequent at the middle third (51%) followed by posterior (39%) and anterior thirds (10%)6 . With regard to the lateral meniscus, it was noted that lesions of the body (middle third) appeared more frequently. In a study on the location of the meniscal injuries , Rico and Ayala (1997) observed that the medial meniscus was more commonly affected and topographical lesions were more frequent at the middle third (51%) followed by posterior (39%) and anterior thirds (10%). With regard to the lateral meniscus, it was noted that lesions of the body (middle third) appeared more frequently6 . Braz and Silva observed that the width and thickness were inversely related, the greater the width thinner was the part, smaller the thickness width was greater. In our study we didn’t observed the same. In our study we found that posterior third of the lateral and medial menisci was the widest part which correlates with the observation of Murlimanju et al., and Almeida etal. There is lower incidence of the injury in the anterior 1/3rd of the meniscus so that it can be assumed that the wider the meniscus, it is more susceptible for injuries. This can be justified by the fact that greater the width of the meniscus, the more it is exposed to the actions of the femoral condyles. In our study also as other studies (Table 3 &4) we found that the anterior 1/3rd of the medial meniscus is the one with smallest width compared with other two points. The peripheral lengths (outer circumference) of the menisci are convex, fixed and attached to the inner surface of the joint capsule. The lateral meniscus is firmly attached to the anterior and posterior tibial intercondylar area and it is posterolaterally grooved by the popliteal tendon, which separates it from the fibular collateral ligament. Thus the mobility of posterior horn of lateral meniscus is controlled by tendon of popliteus and meniscofemoral ligaments.Because of these attachments when compared with the medial side, the lateral meniscus has considerably more average excursion with flexion and extension of the knee. Under normal conditions, the lateral meniscus has as much as 1 cm of motion, whereas the medial meniscus moves only 3 mm which prevents lateral meniscus from getting injured. The inner edge of both the menisci are thin concave and unattached. The comparison of the peripheral length data of the present study with earlier studies is represented in Table 7 & 8. These differences in values might be because of racial variations or due to different methods used. We did not observe any statistically significant differences between peripheral length of medial and lateral menisci as that of Braz and Silva. In this study we found that the inner border length of the medial menisci were significantly higher than the (p< 0.05) the lateral menisci. In contrast, Muralimanju et al., observed no difference in inner border length of medial and lateral menisci. Present study results agree with other studies, (Table9) that the distance between the anterior and posterior horns is less in lateral menisci than those of medial meniscus, due to this fact that the lateral meniscus has the form of an almost complete ring, where as medial is more like a half moon. It can also be explained by larger size of the medial condyle of the tibia, medial meniscus has got bigger distance between its horns, whereas the lateral meniscus has a smaller distance between its horns thus compensating for difference in the size of tibial plateau, which is bordered by the menisci. The greater proximity of the horns of the lateral meniscus may explain why they are less prone to injury8 . In our study we observed little higher incidence of discoid lateral meniscus, because of which the mean value of distance between horns was lesser when compared to other studies (Table 9). Nowadays people are choosing sports as a profession rather than as hobby. As people are participating more in sports chances of getting injury of knee is also increasing particularly in football, soccer, baseball, cricket players. Diagnostic and therapeutic arthroscopy is popularly applied in knee problems. Hence in the present work, an attempt has been made to study the menisci in detail, so that it can throw more light for orthopaedic surgeons either to repair menisci injuries or for allograft meniscal replacement surgeries. The data obtained in the present study can be useful in a sizing algorithm for artificial meniscal implants or in the design of artificial prostheses.
CONCLUSION
In meniscus allograft transplantation, correct size of the allograft is likely to be critical to successful healing and functionality. Accurate measurement of meniscal characteristics would be helpful as a clinical evaluation tool for following meniscal replacement and regeneration techniques. We hope that the parameters which we have been measured in the South Indian cadavers will be helpful for preparing synthetic scaffold of menisci and selecting allograft for menisci transplantation in these populations.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars who articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Standing S. Gray’s Anatomy, The Anatomical Basis of Clinical Practice, 39th edn, Elsevier Limited, London, 2006; 1476- 87.
2. Almeida S.K.S., Demoraes A.S.R, Tashiro T, Neves S.E., Toscano A.E, Deabreu R.RM. Morphometric study of menisci of the knee joint. Int.J.Morphol. 2004; 22(3): 181-4.
3. Murlimanju BV, Morphometric analysis of the menisci of the knee joint in South Indian human fetuses. Int. J. Morphol. 2010; 28(4): 1167-71.
4. Fairbank TJ. Knee joint changes after meniscectomy. J bone Joint Surg B.1948; 30: 664-70. 5. Braz PRP, Silva WG. Meniscus morphometric study in humans. J.morphol.Sci.2010; 27(2):62-6.
6. Rico, E. G. C, Ayala, C. E. A. Localizacion de las rupturas meniscales en nuestro medio. Rev. Mex. Ortop.Traumatol. 1997; 11:10-3,
7. Erbachi H, Gumusburun E, Bayram M, Karakurum G, Sirikei A. The normal menisci: in vivo measurements. Surg Radiol Anat 2004; 26: 28-32.
8. Messner K,Gao J. The menisci of the knee joint. Anatomical and functional characteristics and rationale for clinical treatment. J of Anat.1998; 193:161-178.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





