IJCRR - 5(8), April, 2013
Pages: 113-117
Date of Publication: 25-Apr-2013
Print Article
Download XML Download PDF
STUDY OF THE AZYGOS SYSTEM OF VEINS IN HUMAN CADAVER
Author: Kanchana latha G., Raju Sugavasi
Category: Healthcare
Abstract:Objectives: To investigate the origin, course, relations, tributaries and terminations of azygos system of veins in human cadavers. Methods: A total number of 100 specimens (Foetuses: 10, Children: 8, Adults: 82) were selected for this study. Results: The azygos vein is formed by the union of ascending lumbar vein and subcostal veins in 88% of subjects and subcostal veins alone in 12% of subjects. The termination of azygos vein took place at the level of 4 th thoracic vertebra in 85%, 3rd thoracic vertebra in 8% and 5th thoracic vertebra in 7% of subjects. Conclusions: The anomalies of azygos vein, hemiazygos, and accessory azygos veins are very rare. The variations in the azygos system of veins are utmost importance for thoracic surgeons because vulnerability of damage during surgical procedure.
Keywords: Azygos vein, Foetus, variation, Superior vena cava
Full Text:
INTRODUCTION
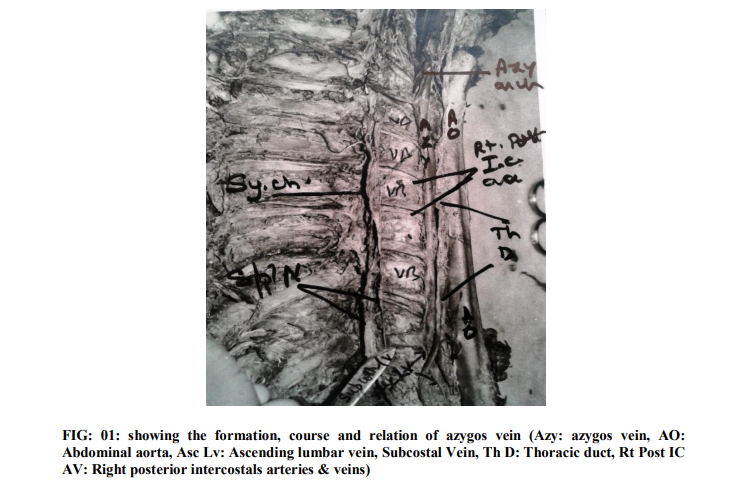
The name azygos derived from Greek, which means unpaired. The Azygos system is a main channel of drainage of the thoracic wall and also part of parities of abdomen. Azygos vein is formed by joining the right ascending lumbar and sub costal veins in posterior mediastinum (FIG: 01).After the formation it passes forward and to the right of the twelfth thoracic vertebra behind the right crus of diaphragm. At the level of the fourth thoracic vertebra, it arches forward above the right pulmonary hilum then it terminates into superior vena cava. The hemi azygos vein is formed by the left ascending lumbar and sub costal veins, and then it ascends upwards ends in azygos vein at the level of eighth thoracic vertebral level. The accessory hemi azygos vein is formed by veins from fourth or fifth to eighth left inter costal spaces, then it crosses the seventh thoracic vertebra to join the azygos vein [1]
MATERIALS AND METHODS
The materials selected for this present study were human cadavers and fetuses. A total number of 100 specimens (TABLE: 01) were obtained from the department of Anatomy, forensic medicine and Gynaecology& Obstetrics of Kurnool medical college, Kurnool, Andhra Pradesh, India. The selected cadavers were preserved by injecting with routine embalming fluid. Cadavers from department of forensic medicine were dissected immediately after the autopsy. Received fetuses were fixed by 10% formalin into the serous and cranial cavities and preserved in embalming tank fluid. The preserved fetuses and cadavers were taken and the thoracic and abdominal cavities are opened by a midline incision from the supra sternal notch to pubic symphysis. The thoracic and abdominal organs were removed by dissection then observed the commencement and termination of azygos vein into superior vena cava. All the posterior intercostal veins are cleaned to the site of their termination into the azygos vein.The communications of the hemiazygos, accessory azygos veins into azygos vein are identify and cleaned by reflecting the oesopagus and aorta.
RESULTS
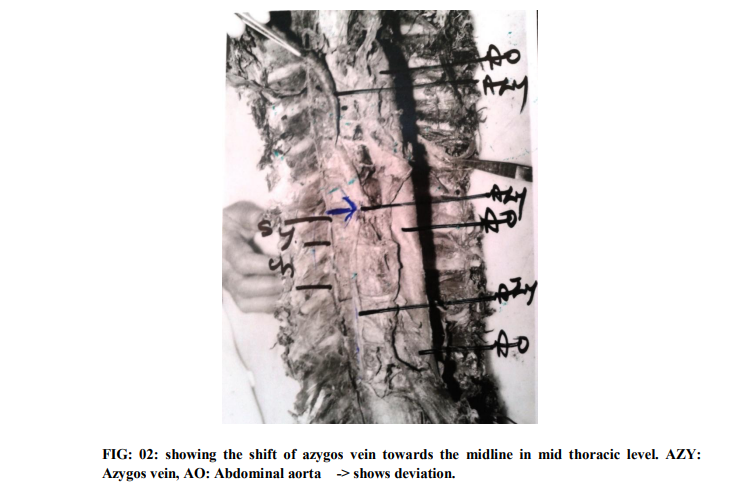
In the present study we concluded the, mode of formation of azygos vein, its deviation and side shifting and its termination related to vertebral level. A total number of 100 specimens, the azygos vein (FIG: 01) formed by the union of ascending lumbar vein and subcostal veins in 88% of subjects, where as it is formed by subcostal veins alone in 12% of subjects (TABLE: 02). Out of 10 foetuses and 8 children the azygos vein was right anterolateral aspect of vertebral bodies. In all adult cadavers up to 45 years age group the azygos vein was located right side, but age group between 45 to 70 years the azygos vein was found to be crossing the midline towards the left side (FIG: 02). In the present study the level of termination of azygos vein into superior vena cava was varying considerably, in adults, fetuses and children. Out of 82 adult cadavers 7 were terminated at third and 75 were at fourth thoracic vertebra. Out of 10 foetuses one at third, two at fourth, and seven at the level of fifth thoracic vertebra. In all the 8 cadavers of children azygos vein terminated at the level of fourth thoracic vertebra (TABLE: 03). Hemiazygos vein is crossing the midline towards the right side at the level of eight thoracic vertebra in 70 % of subjects and at the ninth thoracic vertebra in 3 % of subjects. The formation, course and termination of accessory hemiazygos vein observed normal.
DISCUSSION
Kagami et al [2] studied azygos system of veins in a total number of 26 adult human bodies and 10 foetuses, in 22 out of 26 bodies the azygos vein crosses the midline of vertebral column from right to left, in 3 bodies azygos vein ascending in midline, and one body azygos vein ascending on the right side of vertebra column. ac mahon et al [3] observed the congenital absence of azygos vein, is a cause for aortic nipple enlargement. Lindsay et al [4] reported the abnormal hemiazygos vein. Seib et al [5] conducted a study on azygos system of veins in American whites and Negroes. Gladstone et al [6] conducted study on development of inferior vena cava, he observed the abnormalities in ascending lumbar and azygos vein. Chiiba et al [7] reported a rare case of persistence left azygos vein in a left lung. According to Celik et al [8] anatomical knowledge about the variations of azygos systems of veins are important in radiological diagnosis like CT and MRI techniques and also in the surgical treatment of aneurysms of thoracic aorta and posterior mediastinal tumours. According to Elzbieta Krakowiak Sarnowska et al [9] studies, out of 32 human fetuses the azygos vein situated 90.6% on right side, 9.4 % on median side and the azygos vein terminated at the level of T4 and hemiazygos vein at the level of T7. Kadir et al [10] observed the termination of azygos vein seen at T4, T5 and hemiazygos vein at T7 level. The variations of azygos, hemiazygos, and accessory hemiazygos veins are exisisted in associated with congenital anomalies of the heart, arteries, and veins, like doubling of superior and inferior vena cava. Cotter et al [11] demonstrated double superior vena cava in three human hearts. Mori et al [12] reported double superior vena cava in 2 cases out of 300 Japanese cadavers. Morton et al [13] reported pre aortic anastomotic channel between azygos and hemiazygos veins.
CONCLUSION
Azygos vein was formed by ascending lumbar vein and subcostal veins in 88% of subjects and only by subcostal veins alone in 12%.Termination of azygos vein seen at the T4 level in 85%, T3 level in 8% and T5 level in 7% of subjects. The present study concluded the deviation of azygos vein that was due to ageing basis. The hemiazygos vein crossing to right side at T7 level in 70%, T9 level in 3% of subjects.
ACKNOWLEDGEMENTS
Authors are greatful to Dr. B.T. Narayana Rao, HOD, Department of Anatomy, Kurnool Medical College, AP, India and also previous authors, publishers, editors of all of those articles, journals and books from where the literature of this article has been reviewed and discussed.
References:
1. Standring S. Gray’s Anatomy. The Anatomical basis of clinical practice. 39th ed. Edinburg. Elsevier Churchill Livingstone. 2005; (60):1026 1027.
2. Kagami H, Sakai H. The problems in the arrangements of the azygos vein leftward deviation of azygos vein. Okajimas folia Anat Jap.1990; 67 (2 3):11 4.
3. Mac mahon H. congenital absence of azygos vein: a cause for aortic nipple enlargement. AJR Am J. Roentgenol. 1987; 149 (2): 273 4.
4. Lindsay HC. An abnormal vena Hemiazygos. J Anat. 1925; (50): 438.
5. Seib GB. The azygos system of veins in American whites and American Negroes. AM .J. Phy Anthropol. 1934; 19 39.
6. Gladstone R J. Development of IVC in the light of receat research with spt reference to certain abnormalities and current descriptions of ascending lumbar and azygos veins. J Anat. 1929; (64): 60 93.
7. Chiiba S. An autopsy case of azygos lobe. Okajimas folia Anat.Jap.1990; (66): 313 37.
8. Celik HH, Sargon MF, Aldur MM and Cumbur M. An anomalous course of the interazygos vein. Surg Radiol Anat.196; 18: 61–62.
9. Elzbieta Krakowiak Sarnowska, Marcin Wisniewski, Michal Szpinda, Helena Krakowiak. Variability of the azygos vein system in human fetuses. Folia Morphol. 2003; (62) 4: 427–430.
10. Kadir S. Atlas of normal and variant angiographic anatomy. WB Saunders Company, Philadelphia. 1991; pp. 164–165.
11. MC Cotter RC. Demonstration of 3 human hearts showing double superior vena cava. J Mic. Med Soc. 1915; 14: 479 484.
12. Mori c. Two cases of double SVC Japan heart. J. 1990; (6): 881 8. 13. Morton WRM. Pre aortic drainage of azygos vein report of 2 cases. Anat Rec. 1948; 101 187.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





