IJCRR - 9(1), January, 2017
Pages: 06-08
Date of Publication: 07-Jan-2017
Print Article
Download XML Download PDF
PERIPHERAL OSSIFYING FIBROMA- A CLINICO-HISTOPATHOLOGICAL REPORT
Author: Kalpana Gokul1, Kamala R.2, Basavaraj N. Kallalli3, Jyothi Zingade4
Category: Healthcare
Abstract:Aim: This article attempts to describethe peripheral ossifying fibroma of gingiva in a 40 year old male patient.
Case Report: A 40 year old male patient presented with a growth which was lobulated, sessile, asymptomatic and firm in consistency. Histopathological picture shows hyperparakeratinized epithelium with long and slender rete ridges, with collagen fibresand chronic inflammatory cell infiltrate in connective tissue stroma, suggestive of Peripheral Ossifying Fibroma.
Conclusion: Knowledge of the frequency and presentation of the most common oral lesions with its differential diagnosis is beneficial in developing an early clinical diagnosis of such lesions and its management in the primary stage with minimum surgical intervention.
Keywords: Fibrous hyperplasia, Oral mucosal lesion, Peripheral ossifying fibroma
Full Text:
INTRODUCTION
Oral mucosa is constantly subjected to external and internal stimuli and therefore presents with a spectrum of diseases that range from developmental, reactive, inflammatory and neoplastic.1,2,3 These lesions present as either generalized or localized. Reactive lesions of the gingiva are clinically non-neoplastic nodular swellings that develop in response to chronic and recurrent tissue injury which stimulates an exuberant or excessive tissue response.2,4 They may present as pyogenic granuloma, fibrous epulis, peripheral giant cell granuloma, fibroepithelial polyp, peripheral ossifying fibroma, giant cell fibroma, and pregnancy epulis. Such reactive lesions are less commonly present in other intraoral sites such as cheek, tongue, palate and floor of the mouth but very frequently present in relation to the gingiva.1,2 Clinically, these reactive lesions often present diagnostic challenges because they appear similar. But they possess distinct histo-pathological features.3,4
Here we present a case of peripheral ossifying fibroma manifesting as inflammatory hyperplasia rather than a true neoplastic lesion of connective tissue origin.
CASE REPORT
A 40 year old male patient visited to the department of oral medicine and radiology with the chief complaint of growth in the lower front tooth region of jaw since 5 months. Patient gives history of growth which was smaller in size initially and gradually increased to the present size. He had difficulty while brushing and on mastication. Past dental history revealed he visited to the dentist 5 months back for the same complaint and underwent surgical excision. Patient again noticed small growth after 1 week of excision which gradually increased to the present size. Patient had habit of tobacco chewing 3-4 times/day 10 years back but he quit his habit 3 years back.
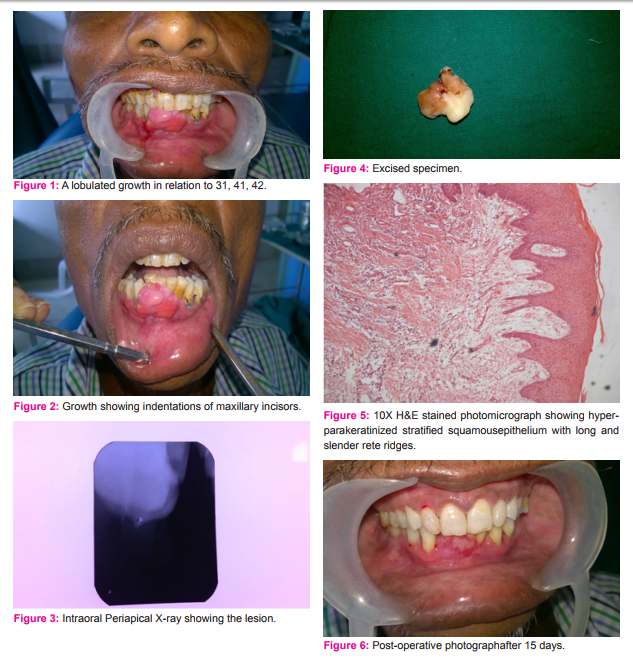
On intraoral examination a single lobulated growth was present on the attached gingiva in relation to 31,32,41 with sessile base. Extending superiorly 2 mm below the incisal edge of 31,41,42 to 2mm above the lower labial vestibule and from mesial of 32 tooth to mesial of 43 measuring about 2x3 cm in size. Overlying mucosa of the growth was, blanched superiorly while the inferior surface was erythematous.Indentations of the 11,12,21 were seen on the superior surface of the growth. No visible surface pulsation, ulcerations, bleeding was seen. On palpation growth was non-tender, firm in consistency and not fixed to the underlying tissue. Bleeding on probing was present. With the history and clinical examination provisional diagnosis was given as Peripheral ossifying fibroma. (Figure 1,2)
An intraoral periapical radiograph showing radiopacities suggestive of calcifications.(Figure 3)
Haematological investigations were carried out, all the values were within the normal limit.
Excisional biopsy of the patient was carried out under local anaesthesia and excised specimen was sent for the histopathological examination. (Figure 4 )
Histopathologically the hematoxylin and eosin stained section revealed hyperparakeratinized stratified squamous epithelium with long and slender rete ridges. Connective tissue stroma showing dense collagen fibres with chronic inflammatory cell infiltration. The overall features suggestive of Peripheral Ossifying Fibroma (Figure 5)
The patient was followed after 15 days, and no recurrence was noticed. (Figure 6)
DISCUSSION
Fibrous growths of the oral soft tissues are fairly common and include a diverse group of reactive and neoplastic conditions. Tissue enlargement of the oral cavity often presents a diagnostic challenge because a diverse group of pathologic processes can produce such lesions.5,6,7 They are categorized into four subgroups which includes pyogenic granuloma, peripheral ossifying fibroma, peripheral giant cell granuloma and fibrous hyperplasia (Kfir et al).10 Fibro epithelial hyperplasias are reactive/ inflammatory conditions and they give rise to variety of lesions named according to their clinical presentation. Most of these lesions arise on gingiva, reflecting universal presence of inflammation in the interdental papillae.1,3
Lesions are associated with local predisposing factor like mal-aligned teeth, ill-fitting restorations, calculus which prevent removal of bacterial plaque and indirectly induce inflammation.2,11 It is interesting that most reactive hyperplastic lesions occurred in the female gender with female to male ratio of 1.5:1. In a study carried out by Zarei et al and Aghbali et al they were more common in females (male to female ration of 1:1.8 and 1: 1.4).Reactive lesions of the gingiva are clinically and histologically non-neoplastic nodular swellings that develop in response to chronic and recurrent tissue injury which stimulates an exuberant or excessive tissue response.10
Peripheral Ossifying Fibroma is a histological variant of fibroma and a proliferative fibrous lesion of the gingival tissue that causes esthetic and functional problems which need to be evaluated and treated as early as possible.4
The clinical aspects of Peripheral Ossifying Fibroma with calcification and ossification are similar to pyogenic granuloma. Yehoshua Kfir et al in his clinicopathologic study conducted on 741 cases it has been proved that Peripheral Ossifying Fibroma with calcification and ossification affects more commonly young people and female.1
Daley et al suggested that the vascular component of pyogenic granuloma is gradually replaced by fibrous tissue with time and hence, diagnosed as a fibrous hyperplasia or fibroma.
Natheer Al- Rawi et al observed that fibrous hyperplasia on the gingiva not only have the same female gender preponderance but occur in the same age group and site as gingival pyogenic granuloma. An inference that fibrous hyperplasia represents a fibrous maturation of pyogenic granuloma especially in lesions with long duration. Fibrous inflammatory hyperplasia may occur on any surface of the oral mucous membrane as either pedunculated or sessile growth. Lesions more than one cm in diameter are rare in cheeks, tongue and floor of the mouth because masticatory stresses restricts their size through necrosis and ulceration.3,4,10
Histopathologically, these lesions shows hyperplastic stratified squamous epithelium, thin finger like rete ridges extend into underlying connective tissue stroma which are fibrocellular. Chronic inflammatory cell infiltrate are seen. These lesions are treated by complete local excision and removal of chronic irritant and low recurrence rate is expected.1,2,5
CONCLUSION
Oral lesions are first detected by oral physicians. Knowledge of the frequency and presentation of the most common oral lesions with its differential diagnosis is beneficial in developing an early clinical diagnosis of such lesions and its management in the primary stage with minimum surgical intervention. Although there is female predominance the present case represents a rare reactive lesion in male. It is difficult to differentiate clinically between pyogenic granuloma, peripheral ossifying fibroma, peripheral giant cell granuloma and fibrous hyperplasia. Hence a histopathological investigation is helpful to arrive at accurate diagnosis.
References:
- Gorwade N, Dhalkari CD, Ambulgekar JR. Inflammatory fibro-epithelial hyperplasia with two variants- A report of three cases. Int. J Sci Res 2014;3:1-2
- Astekar M, Gupta S, Soumya G. Focal Fibrous Hyperplasia: Report of two Cases. Int J Dent Clin 2011;3:111-112
- Suryaprasanna J, Sehrawat S. Fibroepithelial hyperplasia: Rare, self-limiting condition- Two case reports. J Adv Oral Res 2011; 2;70
- Reddy V , Saxena S, Saxena S, Reddy V. Reactive hyperplastic lesions of the oral cavity: A ten year observational study on North Indian Population J Clin Exp Dent 2012;4:e136-40.
- Shafer. Textbook of Oral Pathology. 5ed. New Delhi, Elsevier. 2007:178-180.
- Regezi JA, Sciubba. Connective Tissue Lesions. Oral Pathology: Clinical Pathologic Correlations. 5 ed. St. Louis, Saunders, Elsevier, 2008:155- 178.
- Michael Glick. Burket’s Oral Medicine. People’s Medical publishing house; 12th edition.2015
- Brad W. Neville, Douglas D. Damm, Carl M. Allen, Jerry E. Bouquet. Text book of Oral and Maxillofacial Pathology.2nd edition.
- Jafarzadeh A, Sanatkhani M, Mohtasham N. Oral pyogenic granuloma: a review, J Oral Sci 2006; 48: 167-175.
- Jain K, Singh BD, Dubey A, AvinashA .Fibro-Epithelial Hyperplasia Mimicking Mucocele. Kathmandu Univ Med J 2014;12 :146-148.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





