IJCRR - 5(22), November, 2013
Pages: 64-73
Date of Publication: 04-Dec-2013
Print Article
Download XML Download PDF
DIAGNOSTIC IMAGING OF INTRACRANIAL NEOPLASMS: HOW FREQUENT ARE INDICATIVE FINDINGS IN CT AND MRI?
Author: Ravinder Kumar , Jyoti
Category: Healthcare
Abstract:Objective: This study aims to compare the ability of computed tomography and magnetic resonance imaging for detection, characterization and localization of intracranial neoplasms. Material and Methods: Total 60 cases with clinical suspicion of intracranial neoplasm of all age groups and either sex were evaluated. All MR images were obtained with a 1.5-T superconducting system (SIEMENS) using a circularly polarized head coil. Pre and post contrast CT was done in all cases on 64 Slice Helical Seimens Somatom CT scanner machine. Results: CT proved to be superior in demonstrating calcifications and a typical tumor density. On the other hand, MRI was better suited for identifying the extraaxial location of tumors, the broad contact of tumors to the meninges, tumor capsules and contrast enhancement adjacent to the tumors. Both methods provided nearly equal results in demonstrating mass effects, hyperostoses, intensive and homogeneous contrast enhancement, and smooth tumor contours after contrast administration. On the whole, neither of the two methods demonstrated a universal superiority for the diagnosis of intracranial neoplasms. Rather, each method displayed distinct advantages. Conclusion: Application of a diagnostic algorithm that integrates advanced imaging features with conventional imaging findings may help the practicing radiologist make a more specific diagnosis for an intracranial tumor.
Keywords: Computed tomography, intracranial neoplasm, intratumoral calcification, Magnetic resonance imaging, supratentorial.
Full Text:
INTRODUCTION
Intracranial neoplasms can be detected at an early stage with the help of diagnostic modalities. The goals of diagnostic imaging in the patient with suspected intracranial tumour include:
- Detection of the presence of a neoplasm.
- Localization of the extent of tumour. (Including definition of involvement of key structures and assessment of the presence and severity of secondary changes.)
- Characterization of neoplasm.1
In 1970, CT emerged as primary diagnostic screening modality for the detection of intracranial disease. Areas of structural abnormality appeared on CT as regions of altered tissue radiographic density. Accuracy of localization with CT exceeded the accuracy that could be achieved by cerebral angiography or any other invasive diagnostic procedures.2
Since introduction of Magnetic Resonance Imaging (MRI) as clinically practicable diagnostic modality in 1980, it has rapidly earned recognition as the optimal screening technique for the detection of most intracranial neoplasms. Early experience suggested that 3% to 30% more focal intracranial lesions could be identified on MRI than on CT.
Compared with CT, MRI using spin echo, gradient echo and combination of spin and gradient echo pulsing sequences before and after intravenous administration of paramagnetic contrast agents provides inherently greater contrast resolution between structural abnormalities and adjacent brain parenchyma and has fuelled the development of MR from an in vitro laboratory tool to an in vivo diagnostic instrument. Even with current state of the art equipment utilizing very high magnetic fields and rapidly switching gradient coils, MR nevertheless suffers two disadvantages:
- MRI requires significantly large image acquisition time.
- Abnormalities involving cortical bone, intratumoral calcification and hyperacute haemorrhage are more clearly and accurately assessed with CT.
As both CT and MRI are helpful in the diagnosis of intracranial neoplasms. Hence this study is undertaken to compare the role of computed tomography and magnetic resonance imaging in intracranial neoplasms
MATERIAL and METHODS
Sixty patients with clinical suspicion of intracranial neoplasm attending the various surgical and medicine outpatient departments (OPDs) and wards of our hospital were included in the study.
cOMPUTED TOMOGRAPHY (CT)
Pre and post contrast CT was done in all cases on 64 Slice Helical Seimens Somatom CT scanner machine, time of which is 0.4 seconds.
magnetic RESONANCE IMAGING (MRI)
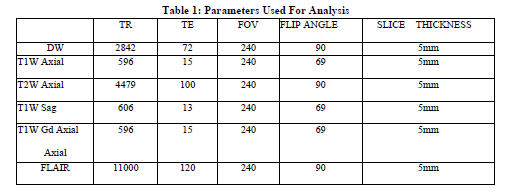
All the studies were conducted on 1.5 Tesla super conducting magnet, SIEMENS, Head coil was used. Parameters used for analysis were shown in Table 1
RESULTS
Sixty cases comprising of various type of primary and secondary neoplasms were studied. Since, metastases showed fewer incidences in our study because most of the patients with a known primary were subjected to one imaging modality either CT or MRI. So, these patients were excluded from the study as our study was based on comparative evaluation of CT and MRI in intracranial neoplasms. Overall observations were following:
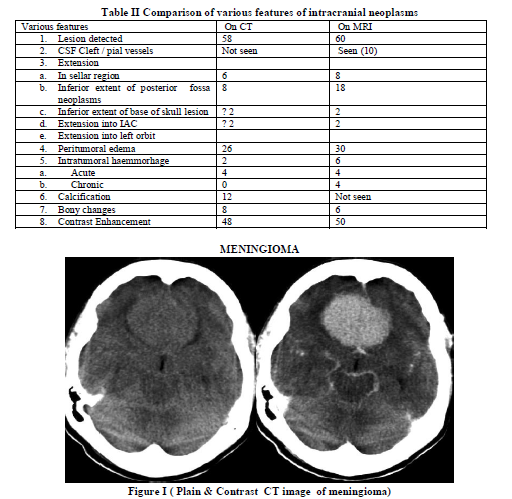
Table II summarizes the general comparison of various features of intracranial neoplasms as follow:
CT failed to demonstrate the lesion in two cases and showed only hydrocephalus whereas MRI showed the lesion in medulla .MRI demonstrated the CSF cleft and pial vessels in 8 out of 10 cases of meningioma and in two cases of dural based metastases and acoustic schwannoma, however these findings were not demonstrated on CT.
Tumor extension into sellar region was noted in 12 cases with MRI while it was observed with 8 cases on CT. There were 18 cases of posterior fossa tumors in our series of 60 cases. MRI displayed the full extent including the inferior extent in 18/18 cases whereas; CT demonstrated the full extent in 10 cases only. In two cases of dural based metastases inferior extent of the base of skull lesion was better demonstrated by MRI.
Extension into internal auditory canal and left orbit in cases of acoustic schwannoma and dural based metastases respectively were better demonstrated on MRI than CT.
MRI showed peritumoral edema in 30 cases while on CT it was observed in 26 cases. Intratumoral hemorrhage was seen in 6 cases with MRI, while on CT it was observed in two cases. CT was able to detect only acute intratumoral hemorrhage while MRI demonstrated both acute and chronic intratumoral haemorrhages.Better demonstration of
acute intratumoral hemorrhage was seen with CT than MRI.
Calcification was noted in 12 cases on CT. MRI failed to depict the calcification in all cases. Bony changes were noted in 8 cases on CT while MRI showed it in6 cases. MRI failed to depict the hyperostosis in a case of meningioma.
MRI showed contrast enhancement in 50 cases while it was observed in 48 cases on CT. CT failed to detect the tumor in two cases in which MRI showed mild enhancement.
Frequency Distribution of Intracranial Neoplasms
Commonest intracranial neoplasms were gliomas (30%), followed by meningioma (16.6%), metastases (10%), medulloblastoma (6.6%) and others.
Age and Sex Distribution of Intracranial Neoplasms
Incidence peaks of gliomas and meningiomas were seen predominantly in 3rd – 4th decade of life. 20% of all intracranial tumour occurred in paediatric age group under 20 years of age. Also we observed one patient presented in Ist decade of life. Men were found to be affected more than women in present study (17:13) except for meningioma with female predominance (1.5:1).
Location Distribution
In present study supratentorial location (40 /60) was found to be more common than infratentorial locations with both CT and MRI. We observed that MRI was more accurate in lesion localisation than CT. In a case of dural based metastases, two out of three metastatic lesions were observed as located infratentorially on CT.Whereas MRI, clearly demonstrated the lesion in supratentorial location on saggital images.
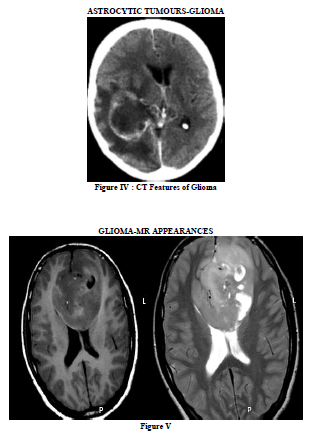
Gliomas
There were eighteen cases of glioma. Most of these were hypodense on NCCT and were hypointense on T1- weighted and hyperintense on T2 – weighted images on MRI. We found that MRI was better in tumour detection, localization, demarcation from normal brain parenchyma, identification of sub acute / chronic intratumoral haemorrhage and degree of enhancement than CT. However, calcification was better seen on CT. (Figure IV and V).
Posterior Fossa Neoplasms
MRI found to be more sensitive than CT.
Meningioma was the most common extra-axial tumour in present study.
MRI provided more information than CT on pituitary morphology and neighbouring structures in sellar, suprasellar, parasellar and juxtasellar neoplasms. MR was superior to CT in assessment of extent of tumour, in demonstration of tumour relationship to vessels, optic chiasma and adjacent structures of brain. (Figure VI). However, CT was superior to MRI in detecting the presence of calcification which is diagnostic in case of craniopharyngioma.
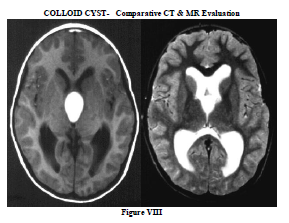
In our two cases of colloid cyst, MR was more sensitive than CT to the presence of tumour and in demonstration of heterogeneity of tumour. (Figure VIII)
In cases of metastases, we made the observation that MR was superior to CT in localisation, assessment of extent of lesion and in degree of enhancement. While, CT demonstrated early intratumoral hemorrhage better than MRI. (Figure VII)
DISCUSSION
Lesion detection:-
McConachie et al4 and Atlas et al1 reported that MR imaging is more sensitive than CT for detection of brain tumors.However, in our study, CT and MRI detected all the cases but in one case of metastasis MRI detected one more lesion.
CSF Cleft / Pial vessels:-
Schubeus et al5 studied fifty cases of meningioma and concluded that MRI appears to be better than CT in demonstrating extraaxial location of the tumour, with the identification of tumour capsule, consisting of CSF margin and displaced vessels and relationship to the meninges.
Similar results were noted in present study as MRI demonstrated the CSF cleft and Pial vessels in eight
out of ten cases of meningioma and in two cases of dural based metastases and acoustic schwannoma, however these findings were not demonstrated on CT. (Figure I, II andIII).
Extent of tumour
Gusnor and Atlas et al 1 reported that MR has the advantage of being able to better define tumour extent than CT because of its greater contrast resolution and multiplanar capability.
Similar results have been found in present study with better demonstration of extent of posterior fossa, base of skull, sellar, parasellar and juxtasella neoplasms on MR than CT.
Peritumoral edema
We observed that FLAIR images showed better demarcation between tumour and edema than conventional MR sequences and CT. In four cases, mild peritumoral edema was seen only on flair images.
Tsuchiya et al also reported the same in their study of 34 patients that FLAIR images showed peritumoral edema more clearly than T2- weighted images when the tumour itself was not hyperintense.
Intratumoral hemorrhage:-
Kieffer and chang described that MRI has greater sensitivity for detection of subacute and chronic haemorrhages whereas early intratumoral or peritumoral haemorrhages are more clearly defined with greater certainty on CT than on MRI.
Similar results were seen in present study, as in two cases where CT failed to detect the intratumoral haemorrhage were found to have subacute / chronic hemmorhage on MRI. In four other cases both CT and MRI showed the early intratumoral haemorrhage but it was more clearly defined with CT than MRI.
Calcification
Lee and Tassel, McConachie et al4 in their studies concluded that CT is highly sensitive in detecting calcification whereas MR cannot reliably demonstrate or exclude its presence. Lovener also found the same that CT is more sensitive than MRI in detecting the presence of calcification. We also observed the same in our study as CT demonstrated calcification in twelve cases whereas MRI was unable to demonstrate it.
Bony changes
Kieffer and Chang, Master and Zimmerman, Yeakley et al reported that CT is superior to MR in demonstration of bone changes like hyperostosis or bone destruction. We also found the same as MRI failed to demonstrate the bony change in a case of meningioma in which CT showed hyperostosis of underlying sphenoid bone. In all other cases, both CT and MRI were equally good in demonstration of bony changes.
Contrast enhancement
Graif et al in their study of seventeen cases of malignant brain tumour compared degree of enhancement with CT and MRI and noted that MRI showed greater degree of enhancement than CT in eight cases. Present study also showed the similar results as MRI showed more enhancement than CT in eight cases, six cases with moderate enhancement and two cases with mild enhancement on CT showed intense enhancement on MRI. In two cases CT was unable to show contrast enhancement while MRI showed mild enhancement.
CONCLUSION
Summarizing, MR has many advantages over CT all without the need of ionizing radiation and iodinated contrast media in imaging of intracranial neoplasms. The multiplanar capability and superior contrast resolution of MRI makes it a better technique than CT in imaging of intracranial neoplasms in terms of tumour detection, localization, assessment of extent of tumour, identification of subacute / chronic intratumoral hemorrhage, degree of enhancement and demonstration of tumour relationship to adjacent structures of brain. MR nevertheless, requires significantly longer image acquisition times than CT. MR is inferior to CT in identification of bony changes, intratumoral calcification and early intratumoral hemorrhage.
Hence, we conclude that MR is the preferable method for evaluation of intracranial neoplasms and CT is useful as a supplementary modality when detailed information about bony anatomy and calcification is required. Also application of a diagnostic algorithm that integrates advanced imaging features with conventional imaging findings may help the practicing radiologist make a more specific diagnosis for an intracranial tumour.
ACKNOWLEDGEMENT
We acknowledge to Geetanjali Medical College and Hospital for their immense support.
Conflict of Interest: None declared


References:
- Atlas SW, editor. Magnetic Resonance Imaging of the Brain and Spine .3rd ed. Philadelphia. Lippincott Williams and Wilkins; 2002.p 695-72.
- Lafitte F, Morel-Precetti S, Martin-Duverneuil N, Guermazi A, Brunet E, Heran F. Multiple glioblastomas: CT and MR features. Eur Radiol. 2001;11(1):131-6.
- John R. Haaga MD, Daniel Boll et al CT and MRI of the Whole Body, 2-Volume Set, 5ed (Computed Tomography and Magnetic Resonance Imaging of the Whole body. P.246-45
- N S McConachie,B S Worthington, E J Cornford, M Balsitis, R W Kerslake, and T Jaspan.Computed tomography and magnetic resonance in the diagnosis of intraventricular cerebral masses Br J Radiol March 1994 67:223-24.
- P. Schubeus, W. Schörner, C. Rottacker, B. Sander . Intracranial meningiomas: How frequent are indicative findings in CT and MRI? Neuroradiology December 1990, Volume 32, Issue 6, pp 467-473
- Allen JC, Siffert J, Hukin J (1998) Clinical manifestations of childhood ependymoma: a multitude of syndromes. Pediatr Neurosurg 28:49–55
- Armington WG, Osborn AG, Cubberley DA, Harnsberger HR, Boyer R, Naidich TP, Sherry RG (1985) Supratentorial ependymoma: CT appearance. Radiology 157:367–372.
- Barkovich AJ (2005) Pediatric neuroimaging. Lippincott, Williams and Wilkins, London.
- Blaser SI, Harwood-Nash DC (1996) Neuroradiology of pediatric posterior fossa medulloblastoma. J Neurooncol 29:23–34
- Brody AS, Frush DP, Huda W, Brent RL (2007) Radiation risk to children from computed tomography. Pediatrics 120:677–682.
- Freilich RJ, Krol G, DeAngelis LM (1995) Neuroimaging and cerebrospinal fluid cytology in the diagnosis of leptomeningeal metastasis. Ann Neurol 38:51–57.
- Koeller KK, Sandberg GD (2002) from the archives of the AFIP. Cerebral intraventricular neoplasms: radiologic–pathologic correlation. Radiographics 22:1473–1505.
- Kramer ED, Rafto S, Packer RJ, Zimmerman RA (1991) Comparison of myelography with CT follow-up versus gadolinium MRI for subarachnoid metastatic disease in children. Neurology 41:46–50.
- Lefton DR, Pinto RS, Martin SW (1998) MRI features of intracranial and spinal ependymomas. Pediatr Neurosurg 28:97–105.
- Maksoud YA, Han YS, Engelhard HH (2002) Intracranial ependymomas. Neurosurg Focus 13(3):1–5.
- Mermuys K, Jeuris W, Vanhoenacker PK, Van Hoe L, D'Haenens P (2005) Best cases from the AFIP: supratentorial ependymoma. Radiographics 25:486–490.
- Nagib MG, O'Fallon MT (1996) Posterior fossa lateral ependymoma in childhood. Pediatr Neurosurg 24:299–305.
- Oppenheim JS, Strauss RC, Mormino J, Sachdev VP, Rothman AS (1994) Ependymomas of the third ventricle. Neurosurgery 34:350–352, discussion 352–353.
- Packer RJ, Siegel KR, Sutton LN, Litmann P, Bruce DA, Schut L (1985) Leptomeningeal
- dissemination of primary central nervous system tumours of childhood. Ann Neurol 18:217–221.
- Qian X, Goumnerova LC, De Girolami U, Cibas ES (2008) Cerebrospinal fluid cytology in patients with ependymoma: a bi-institutional retrospective study. Cancer 114:307–314.
- Ragel BT, Townsend JJ, Arthur AS, Couldwell WT (2005) Intraventricular tanycytic ependymoma: case report and review of the literature. J Neurooncol 71:189–193.
- Rezai AR, Woo HH, Lee M, Cohen H, Zagzag D, Epstein FJ (1996) Disseminated ependymomas of the central nervous system. J Neurosurg 85:618–624.
- Rumboldt Z, Camacho DL, Lake D, Welsh CT, Castillo M (2006) Apparent diffusion coefficients for differentiation of cerebellar tumours in children. AJNR Am J Neuroradiol 27:1362–1369.
- Salazar OM (1983) A better understanding of CNS seeding and a brighter outlook for postoperatively irradiated patients with ependymomas. Int J Radiat Oncol Biol Phys 9:1231–1234.
- Steinbok P, Hentschel S, Cochrane DD, Kestle JR (1996) Value of postoperative surveillance imaging in the management of children with some common brain tumours. J Neurosurg 84:726–732.
- Swartz JD, Zimmerman RA, Bilaniuk LT (1982) Computed tomography of intracranial ependymomas. Radiology 143:97–101.
- Uematsu Y, Hirano A, Llena JF (1988) Electron microscopic observations of blood vessels in ependymoma. Neurol Surg 16:1235–1242.
- Wiener MD, Boyko OB, Friedman HS, Hockenberger B, Oakes WJ (1990) False-positive spinal MR findings for subarachnoid spread of primary CNS tumour in postoperative pediatric patients. AJNR Am J Neuroradiol 11:1100–1103.
- Wootton-Gorges SL, Foreman NK, Albano EA, Dertina DM, Nein PK, Shukert B, Cesario KB, Gage S, Rumack CM, Strain JD (2000) Pattern of recurrence in children with midline posterior fossa malignant neoplasms. Pediatr Radiol 30:90–93.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





